Mesenchymal Stromal Cell (MSC) – Mediated Pain Modulation Mechanisms in Osteoarthritis
Mechanisms at the Joint, Peripheral, and Central Nervous System
Pain is one of the most common clinical signs of osteoarthritis (OA) and can significantly reduce mobility and quality of life. Mesenchymal stromal/stem cells (MSCs) are increasingly being used to treat OA and have demonstrated benefits in reducing OA-associated pain in both veterinary and human clinical trials. So how do MSCs modulate pain?
Research shows that MSCs modulate pain through coordinated, multilevel mechanisms that operate at the affected tissue, the peripheral nervous system, and the central nervous system. Critically, the dominant mode of MSC analgesic action is paracrine, and their therapeutic effects are delivered through secreted cytokines, growth factors, and extracellular vesicles that can result in durable analgesia.1,2 This explains why MSC therapy can produce sustained pain relief in OA and neuropathic pain models without the need for long-term cell survival.
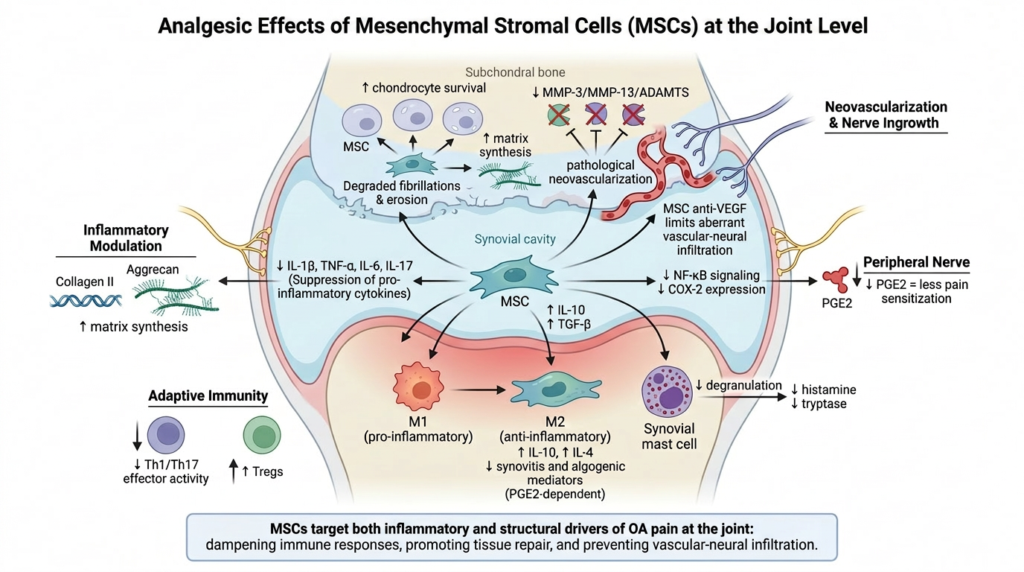
Analgesia at the Joint Level
At the level of the joint, MSCs target the inflammatory and structural drivers of OA pain. They secrete IL-10 and TGF-β, suppressing the pro-inflammatory cytokines (IL-1β, TNF-α, IL-6, IL-17) that sensitize joint nociceptors, and they downregulate NF-κB signaling and COX-2 expression, reducing prostaglandin E2 (a key peripheral pain sensitizer) in the synovium and cartilage.1–3 Joint macrophages are reprogrammed from the pro-inflammatory M1 phenotype to the anti-inflammatory M2 phenotype, with the resulting M2-dominant population producing IL-10 and IL-4 and reducing synovitis and algogenic mediator burden, a process now established to be PGE2-dependent and to occur across multiple inflammatory tissues.4,5 MSCs also suppress synovial mast cell degranulation (reducing histamine and tryptase release), inhibit Th1 and Th17 effector T-cell activity, and expand regulatory T cells (Tregs), collectively dampening the adaptive and innate immune contribution to joint pain.6,7 Structurally, MSCs promote chondrocyte survival, stimulate cartilage matrix synthesis (collagen II, aggrecan), and inhibit MMP-3, MMP-13, and ADAMTS-mediated cartilage degradation, addressing the structural drivers that maintain chronic OA pain.1,8,9 An important emerging mechanism is regulation of pathological neovascularization in osteochondral tissue: pathological new vessels in OA cartilage are accompanied by ectopic sensory nerve ingrowth into normally avascular cartilage, and MSC anti-VEGF effects may limit this aberrant vascular-neural infiltration that contributes to deep joint pain.10
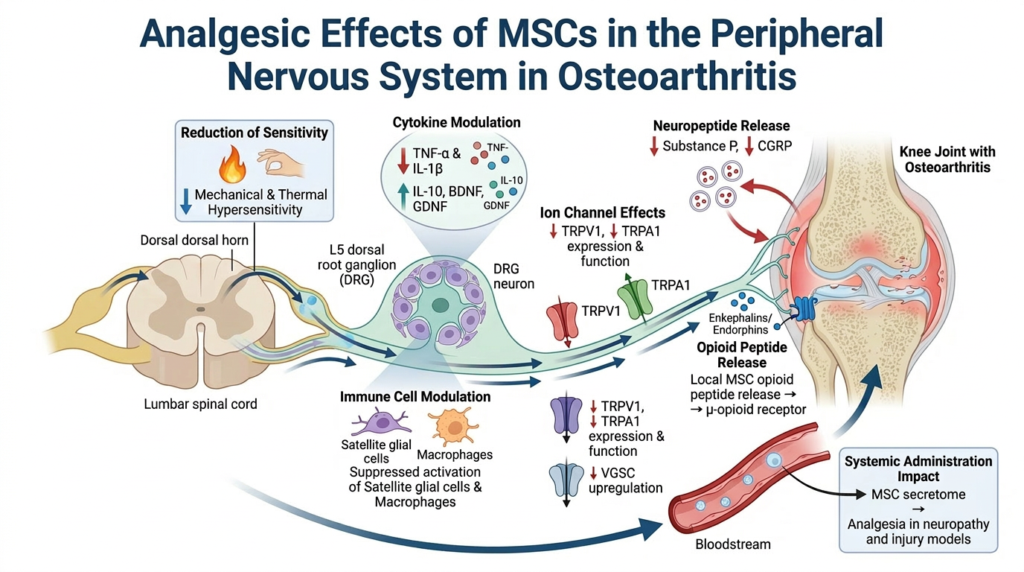
Analgesia within the Peripheral Nervous System
At the peripheral nervous system level, MSCs act directly on dorsal root ganglion (DRG) neurons and peripheral nociceptor terminals. Intrathecal infusion of human umbilical cord MSC-derived exosomes in mice demonstrated localization to the L5 spinal dorsal horn, DRG, and peripheral sensory axons, where they reduce mechanical and thermal hypersensitivity, suppress activation of satellite glial cells and DRG-resident macrophages, and decrease TNF-α and IL-1β while increasing IL-10, brain-derived neurotrophic factor (BDNF), and glial cell line-derived neurotrophic factor (GDNF) in the ipsilateral DRG.11 MSC therapy reduces the sensory afferent expression and function of TRPV1 and TRPA1 channels (ion channels within the joint nociceptor that sense pain), decreases substance P and calcitonin gene-related peptide (CGRP) release from peripheral terminals (primary neuropeptides involved in pain), and may inhibit the upregulation of voltage-gated sodium channels involved in nociceptor hyperexcitability.12,13 Some preclinical evidence demonstrates that MSCs can locally release endogenous opioid peptides (enkephalins and endorphins) that act on peripheral μ-opioid receptors on nociceptor terminals.14 Finally, systemic administration of MSCs reverses nociceptive hypersensitivity in chronic constriction injury and diabetic neuropathy models, with the secretome alone reproducing the analgesic effect, confirming that direct cellular contact with peripheral nerves is not required.12,13
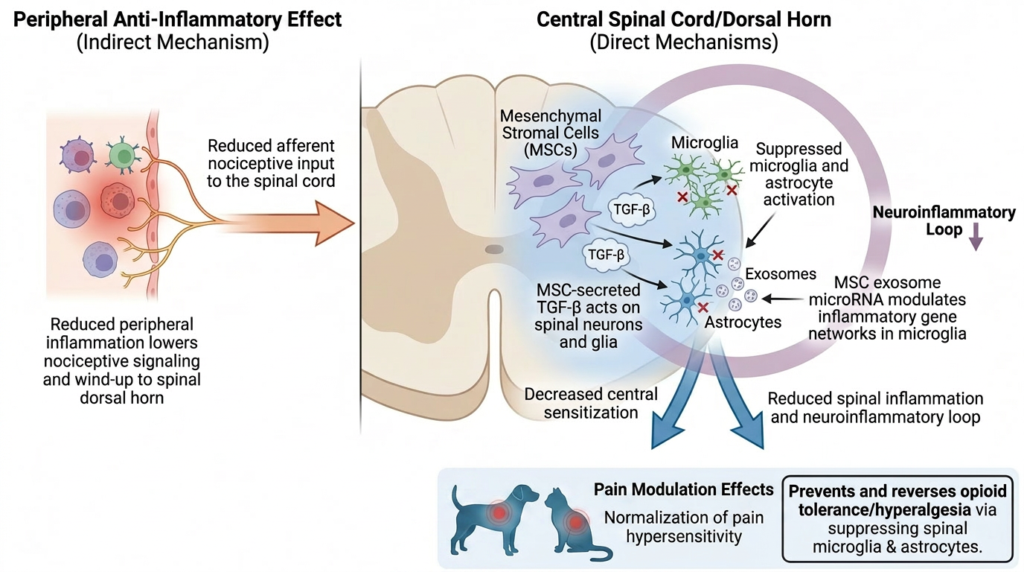
Analgesia within the Central Nervous System
At the central nervous system, MSCs attenuate spinal-cord-level central sensitization through indirect and direct mechanisms. Indirectly, the peripheral anti-inflammatory effects above reduce the afferent nociceptive input that drives wind-up and central sensitization in the spinal dorsal horn.1,14 Directly, MSCs suppress microglial and astrocyte activation in the dorsal horn, with the analgesic effect mediated in significant part by MSC-secreted TGF-β acting on spinal neurons and glia.15,16 MSCs administered intrathecally in peripheral nerve injury models reduce spinal inflammation, normalize pain hypersensitivity, and attenuate the neuroinflammatory loop that maintains chronic pain states.16,17 Notably, MSC transplantation prevents and reverses both opioid tolerance and opioid-induced hyperalgesia in rodent models, with the effect linked to suppression of spinal microglia and astrocyte activation, establishing MSC therapy as a candidate adjunct to chronic opioid use.18 MSC-derived exosome microRNA cargo modulates inflammatory gene networks in spinal microglia without requiring direct MSC engraftment, providing a mechanistic explanation for sustained central effects after therapy.8,11
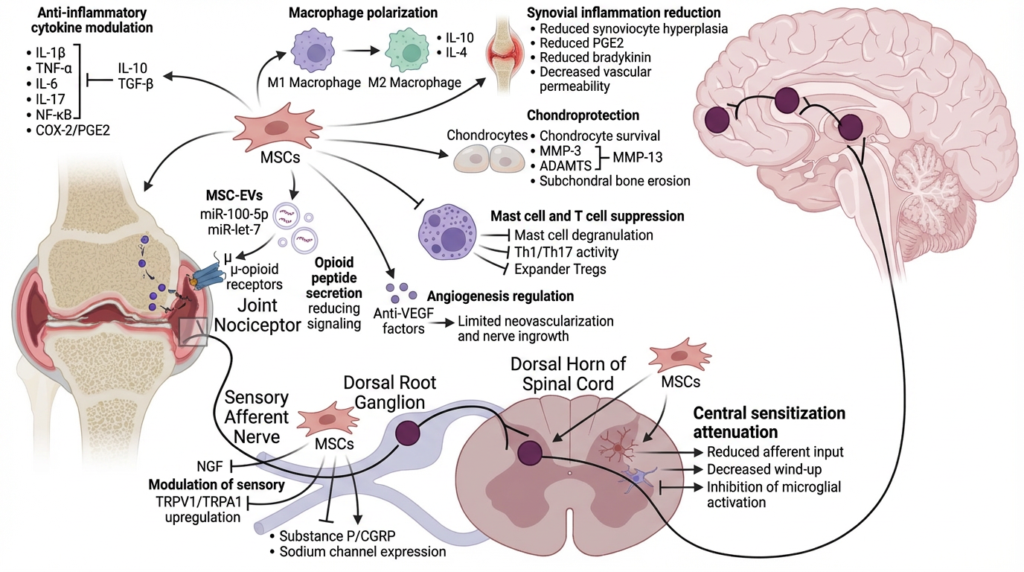
Conclusion
Taken together, MSC-mediated pain control should not be understood as a single mechanism but as a layered, integrated effect: the joint receives anti-inflammatory and structural support; peripheral nociceptors and DRG neurons are de-sensitized through cytokine modulation, ion channel regulation, and local opioid release; and the spinal cord experiences both reduced afferent drive and direct suppression of glial activation. These demonstrated analgesic effects suggest that MSC therapy has the potential to improve pain control and quality of life even before measurable tissue healing or regenerative changes are observed.
References
- Molnar V, Pavelić E, Vrdoljak K, et al. Mesenchymal Stem Cell Mechanisms of Action and Clinical Effects in Osteoarthritis: A Narrative Review. Genes. 2022;13(6):949. doi:10.3390/genes13060949
- Zhang X, Liu T, Ran C, et al. Immunoregulatory paracrine effect of mesenchymal stem cells and mechanism in the treatment of osteoarthritis. Front Cell Dev Biol. 2024;12:1411507. doi:10.3389/fcell.2024.1411507
- Manferdini C, Maumus M, Gabusi E, et al. Adipose‐Derived Mesenchymal Stem Cells Exert Antiinflammatory Effects on Chondrocytes and Synoviocytes From Osteoarthritis Patients Through Prostaglandin E2. Arthritis & Rheumatism. 2013;65(5):1271-1281. doi:10.1002/art.37908
- Németh K, Leelahavanichkul A, Yuen PST, et al. Bone marrow stromal cells attenuate sepsis via prostaglandin E2–dependent reprogramming of host macrophages to increase their interleukin-10 production. Nat Med. 2009;15(1):42-49. doi:10.1038/nm.1905
- Vasandan AB, Jahnavi S, Shashank C, Prasad P, Kumar A, Prasanna SJ. Human Mesenchymal stem cells program macrophage plasticity by altering their metabolic status via a PGE2-dependent mechanism. Sci Rep. 2016;6(1):38308. doi:10.1038/srep38308
- Brown JM, Nemeth K, Kushnir‐Sukhov NM, Metcalfe DD, Mezey E. Bone marrow stromal cells inhibit mast cell function via a COX2‐dependent mechanism. Clin Experimental Allergy. 2011;41(4):526-534. doi:10.1111/j.1365-2222.2010.03685.x
- Aggarwal S, Pittenger MF. Human mesenchymal stem cells modulate allogeneic immune cell responses. Blood. 2005;105(4):1815-1822. doi:10.1182/blood-2004-04-1559
- Toh WS, Lai RC, Hui JHP, Lim SK. MSC exosome as a cell-free MSC therapy for cartilage regeneration: Implications for osteoarthritis treatment. Seminars in Cell & Developmental Biology. 2017;67:56-64. doi:10.1016/j.semcdb.2016.11.008
- Wang R, Xu B, Xu H. TGF-β1 promoted chondrocyte proliferation by regulating Sp1 through MSC-exosomes derived miR-135b. Cell Cycle. 2018;17(24):2756-2765. doi:10.1080/15384101.2018.1556063
- Mapp PI, Walsh DA. Mechanisms and targets of angiogenesis and nerve growth in osteoarthritis. Nat Rev Rheumatol. 2012;8(7):390-398. doi:10.1038/nrrheum.2012.80
- Shiue SJ, Rau RH, Shiue HS, et al. Mesenchymal stem cell exosomes as a cell-free therapy for nerve injury–induced pain in rats. Pain. 2019;160(1):210-223. doi:10.1097/j.pain.0000000000001395
- Brini AT, Amodeo G, Ferreira LM, et al. Therapeutic effect of human adipose-derived stem cells and their secretome in experimental diabetic pain. Sci Rep. 2017;7(1):9904. doi:10.1038/s41598-017-09487-5
- Sacerdote P, Niada S, Franchi S, et al. Systemic Administration of Human Adipose-Derived Stem Cells Reverts Nociceptive Hypersensitivity in an Experimental Model of Neuropathy. Stem Cells and Development. 2013;22(8):1252-1263. doi:10.1089/scd.2012.0398
- Ren K, Vickers R, Murillo J, Ruparel NB. Revolutionizing orofacial pain management: the promising potential of stem cell therapy. Front Pain Res (Lausanne). 2023;4:1239633. doi:10.3389/fpain.2023.1239633
- Chen G, Park CK, Xie RG, Ji RR. Intrathecal bone marrow stromal cells inhibit neuropathic pain via TGF-β secretion. J Clin Invest. 2015;125(8):3226-3240. doi:10.1172/JCI80883
- Schäfer S, Berger JV, Deumens R, Goursaud S, Hanisch UK, Hermans E. Influence of intrathecal delivery of bone marrow-derived mesenchymal stem cells on spinal inflammation and pain hypersensitivity in a rat model of peripheral nerve injury. J Neuroinflammation. 2014;11(1):157. doi:10.1186/s12974-014-0157-8
- Yousefifard M, Nasirinezhad F, Shardi Manaheji H, Janzadeh A, Hosseini M, Keshavarz M. Human bone marrow-derived and umbilical cord-derived mesenchymal stem cells for alleviating neuropathic pain in a spinal cord injury model. Stem Cell Res Ther. 2016;7(1):36. doi:10.1186/s13287-016-0295-2
- Hua Z, Liu L, Shen J, et al. Mesenchymal Stem Cells Reversed Morphine Tolerance and Opioid-induced Hyperalgesia. Sci Rep. 2016;6(1):32096. doi:10.1038/srep32096

Vice President of Veterinary Affairs at Gallant
Dr. Rebecca Windsor, DVM, DACVIM, is a board-certified veterinary neurologist with over 20 years of clinical experience and a strong record of scientific publication. She joined Gallant in 2025 and serves as Vice President of Veterinary Affairs.
Dr. Windsor specializes in veterinary regenerative medicine, with a focus on advancing FDA-approved, off-the-shelf mesenchymal stem cell therapies for pets. She develops educational platforms that translate the science, safety, and clinical efficacy of stem cell therapy for veterinary professionals. Since 2019, she has served as a Clinician Scientist at Ethos Discovery, where she leads the neurology research portfolio.