FCGS Educational Series Part 2: Managing FCGS—Historical Treatment Approaches
This is Part 2 of our three-part Educational Series on Feline Chronic Gingivostomatitis (FCGS).
- Read Part 1: What Causes FCGS? Understanding the Roots of a Debilitating Disease
- Read Part 3: Understanding Mesenchymal Stromal Cell (MSC) Therapy for Refractory FCGS
For veterinarians and cat parents navigating a diagnosis of feline chronic gingivostomatitis (FCGS), the conversation about treatment can feel overwhelming. This is a disease without a single, universally effective solution, and response to treatment can vary between cats. Instead, managing FCGS typically requires a stepwise approach that begins with surgery and may evolve to include medications and mesenchymal stromal cell (MSC) therapy in cats with refractory FCGS. Understanding what each option offers, and what its limitations are, is essential to setting realistic expectations and supporting informed, shared decision-making. For many cat parents, this stage of the journey can feel especially difficult, balancing the desire to relieve their cat’s pain with uncertainty about the right path forward.
In this part 2 of our FCGS educational series, we walk through the historical treatment toolkit: tooth extraction, oral immunosuppressives, anti-inflammatories, antivirals, and other
adjunctive strategies. Mesenchymal stromal cell therapy for refractory FCGS will be covered
extensively in Part 3: Understanding Mesenchymal Stromal Cell Therapy for Refractory FCGS.
How FCGS Shows Up at Home
For many cats, FCGS causes observed changes in behavior, not just visible oral disease.
Cat parents may notice:
- Eating more slowly or walking away from food
- Dropping food or chewing differently
- Reduced grooming or coat changes
- Becoming quieter, hiding more, or interacting less
These changes are communication. They can reflect pain and general systemic discomfort, even when the mouth cannot be easily examined at home.
Tooth Extraction: Initial Management of FCGS
When FCGS is diagnosed, the first recommended treatment is surgical removal of diseased teeth and their associated roots. The rationale is biological: the teeth and their surrounding periodontal pockets serve as the primary reservoir for the bacterial and viral antigens that drive the chronic immune response. By eliminating this antigenic challenge, extraction removes a major source of antigenic stimulation fostering the inflammatory cascade.
Current guidelines and systematic reviews support either partial-mouth extraction (PME) or full-mouth extraction (FME) as the standard of care for FCGS.1–3 FME, which involves removal of all teeth, is generally preferred when disease is severe and widespread, while PME may be appropriate in selected patients with more focal disease. The 2025 Feline VMA oral health guidelines reinforce this recommendation.3
What Does the Evidence Say About Success Rates?
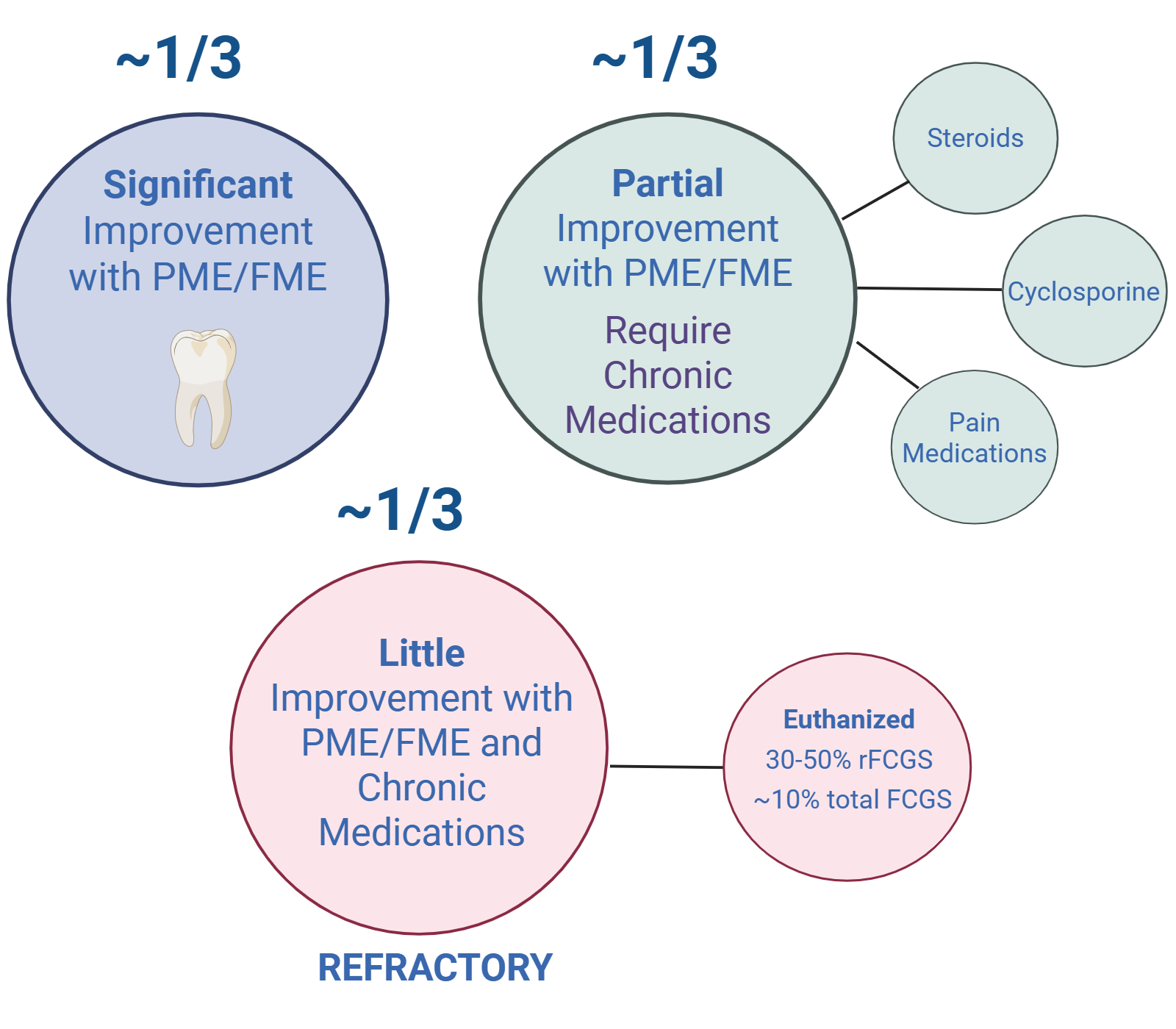
A landmark study evaluated the effect of tooth extraction in 95 cats with stomatitis and found that 28% achieved complete resolution and an additional 40% experienced substantial improvement, for a combined response rate of approximately 68%.4 A 2021 retrospective of 57 cats with FCGS reported that 42.1% achieved complete remission following extraction and 28.1% showed moderate improvement.5
However, the data also consistently show that approximately 1/3 of cats remain refractory to extraction alone and require ongoing medical management.1,2 These cats do not fail because surgery was performed incorrectly—they fail because their immune dysregulation has become autonomous, no longer dependent on the original microbial or viral trigger. In these patients, extraction is a necessary but insufficient intervention.
Factors That Affect Extraction Outcomes
Not all cats respond equally. Several factors are associated with worse outcomes after extraction:
- Sustained immune dysregulation after the diseased teeth and other potential factors are addressed
- Retroviral disease: FeLV-positive cats are 7.5 times more likely to show no improvement after extraction.6 A case series examining cats with concurrent FCGS and retroviral disease confirmed that these patients experience significantly worse outcomes, with lingual ulcers serving as an independent predictor of poor response—and FeLV cats tend to have more lingual ulcers.
- Lingual ulcers: Cats with lingual ulcers, regardless of retroviral status, are 2.7 times more likely to have a worse response to extraction.6
- Timing: Spontaneous recovery from FCGS has never been reported, and outcomes worsen the longer the disease goes without appropriate intervention.2
A 2025 study on the prevalence of reasons for tooth extraction in cats further highlights that FCGS is one of the leading indications for extraction in feline dentistry, underscoring both the frequency of the disease and how commonly surgery is required.7
The idea of removing your cat’s teeth can feel alarming and emotional. But cats adapt remarkably well to life after extraction. The goal is to eliminate the source of chronic pain and immune stimulation. Most cats eat normally after recovery—often better than before, because they are no longer in constant pain. The surgery itself is performed under anesthesia, and with appropriate pain management, recovery is typically smooth. Cats are highly adaptive as a species, and many experience meaningful improvements in comfort, behavior, and quality of life following extraction.
Medical Therapies
The following described medical therapies have clinical trial data describing their use for FCGS. Therapies being used without scientific evidence to support their use in cats with FCGS are generally not supported by the veterinary dentistry community and are not described here. Note that pain management (i.e. gabapentin or pregabalin, buprenorphine) is a crucial component to FCGS management; however, specific pain medications are not discussed here.
Oral Immunosuppressive Medications
In cats that remain refractory after extraction—or in cases where surgery is not immediately possible—immunosuppressive medications are the most employed medical strategy. The rationale for immunosuppression in FCGS is direct: because the disease is driven by a dysregulated immune response, dampening that response can reduce tissue-damaging inflammation. Two drugs have the most evidence base: corticosteroids and cyclosporine. In cats, ongoing inflammation can affect not only physical comfort but also behavior, appetite, and interactions, making consistent management especially important.
Corticosteroids
Corticosteroids—most commonly prednisolone—have historically been a first-line medical approach in FCGS. They work through broad immunosuppression, reducing the cytokine cascade and limiting T cell activity that drives mucosal inflammation. In the short term, many cats experience reduction in oral pain and improved appetite.
However, the evidence for long-term efficacy is important to understand. In a randomized, multi-center, controlled double-blind study comparing corticosteroids to interferon omega and placebo, corticosteroids produced substantial improvement in only 23% of cats and clinical remission in just 7%.8 These numbers highlight the limited ceiling of corticosteroid therapy in FCGS—while the drugs can make cats more comfortable in the short term, they rarely lead to resolution of disease.
The side effect profile of long-term steroid use is also a significant concern. Prolonged corticosteroid administration in cats carries risks of iatrogenic diabetes mellitus, immunosuppression predisposing to infections, weight gain, and skin fragility. For this reason, most current guidelines do not recommend corticosteroids as a long-term standalone treatment for FCGS. 1,2
Corticosteroids can provide meaningful short-term palliation for cats in significant pain, but their low remission rate and side effect profile make them a bridge rather than a destination. If a cat is on long-term steroids for FCGS without being evaluated for extraction or other options, it is worth revisiting the treatment plan.
Cyclosporine
Cyclosporine has emerged as the most effective oral immunosuppressive for FCGS. It works through a more targeted mechanism than corticosteroids, primarily inhibiting calcineurin and thereby suppressing T cell activation, addressing the T cell-driven pathology at the heart of FCGS.
A randomized, placebo-controlled, double-blinded study evaluating cyclosporine in cats with chronic, refractory stomatitis demonstrated a higher response rate to cyclosporine compared to corticosteroids: 77.8% of treated cats showed improvement, and clinical cure was achieved in 45.5% of cats treated for more than three months.9
A more recent long-term study evaluated the efficacy of cyclosporine and interferon-ω using Stomatitis Disease Activity Index (SDAI) scores. This study confirmed that cyclosporine provided sustained clinical improvement in FCGS, and provided comparative data against interferon that helped contextualize treatment choices.10
Despite promising efficacy in some cats, discontinuation of cyclosporine occurs most commonly due to challenges with administration and side effects.11 One study reported consistent administration of cyclosporine oral liquid was considered difficult or impossible in 57% of cats.11 The most commonly reported side effects of cyclosporine in cats include vomiting and lethargy/depression, which can limit tolerability in some patients.2,12 One recent study documented side effects in 60% of cats receiving oral cyclosporine solution, including altered behavior in 64% of cats, a previously underrecognized symptom.11 Changes in behavior, including reduced activity or altered interaction, may reflect both medication effects and underlying disease, and should be evaluated in the context of the whole cat.
The FDA label warns cyclosporine may cause elevated levels of serum glucose, creatinine, and urea nitrogen, and should be used with caution in cases with diabetes mellitus or renal insufficiency. Cyclosporine should be administered consistently for best results, which can be challenging in cats with persistent oral pain associated with FCGS. Monitoring for opportunistic infections is advisable given the degree of immunosuppression. Whole-blood cyclosporine levels >300 ng/mL are associated with the most significant clinical improvement, therefore cyclosporine blood level monitoring is recommended.9 Cyclosporine may lose efficacy in some cats over time.1
When initiating cyclosporine for FCGS, set realistic expectations with owners. The drug may take several weeks to months to take full effect. The dosing and side effect profile limits consistent use in some cats. For cats also receiving other immunomodulatory medications, be mindful of additive immunosuppression risk. Cyclosporine requires consistent dosing to maintain its immunosuppressive effect, and routine bloodwork monitoring and cyclosporine levels are recommended. In many cats, cyclosporine can control but not cure disease.
Antiviral Therapies: Recombinant Feline Interferon-Omega (rFeIFN-ω)
Given the strong association between FCGS and feline calicivirus (FCV), targeting the viral component of the disease has been a logical therapeutic focus. Recombinant feline interferon-omega (rFeIFN-ω) has been the most studied antiviral approach in FCGS to date.
Interferon-omega acts by inhibiting viral replication and modulating some innate immune responses, but it has limited effect on acquired immune responses (i.e. regulating T helper cell balance).13 The effect on cytokine modulation appears to be limited to variable effect on IL-6 alone.13
Evidence for Efficacy
A randomized, multi-center, controlled, double-blind study in 39 calicivirus-positive cats with refractory caudal stomatitis were treated with rFeIFN-ω, corticosteroids, or placebo. rFeIFN-ω produced substantial improvement in 45% of cats and clinical cure in 10%—outperforming placebo and showing similar overall efficacy to corticosteroids, with a statistically significant advantage in pain scores at days 60 and 90.8
Another study evaluated a subcutaneous low-dose rFeIFN-ω protocol specifically in FCV-positive cats and found that subcutaneous administration may improve stomatitis by inhibiting FCV proliferation, suggesting that route and dosing protocol influence outcomes.14
Another study specifically asked whether interferon-ω reduces clinical signs more rapidly than steroid treatment and found that neither agent showed a clear speed advantage, reinforcing that FCGS management is generally measured in weeks to months rather than days.15
Availability and Practical Considerations
Although rFeIFN-ω may be effective for some cats with viral-associated FCGS, it is unlikely to show benefit in viral-negative cats and does not address the underlying complex immune dysregulation that it is the hallmark of FCGS.
An important practical caveat: rFeIFN-ω is not currently available or approved for use in the United States. It is available in Europe and some other markets (marketed as Virbagen Omega, Virbac) but US veterinarians do not have routine access to this treatment.
For practitioners in the US, rFeIFN-ω is not a currently accessible option.
Antibiotics
Although antibiotics are sometimes prescribed for FCGS, current evidence does not support their use as a primary treatment and raises concerns about antimicrobial resistance (AMR). One study evaluating the use of amoxicillin and metronidazole in cats with FCGS showed transient improvement in a little over 1/3 of cats. 16 Another study documented the occurrence of AMR genes in the oral microbiome of cats with FCGS, suggesting that repeated antibiotic exposure in these patients may contribute to selection of resistant organisms.17 Given the lower response rate compared to immunosuppressives and concern for AMR, antibiotic therapy is currently only recommended in the acute setting or if secondary infections are indentified.2
Additional Adjunctive Supportive Therapies
Beyond surgery and the primary immunosuppressive or antiviral medications, a growing body of evidence supports the use of adjunctive treatments that address specific components of FCGS pathology. While none of these has been established as a standalone curative therapy, several show promise as additions to a comprehensive management plan.
Omega-3 Fatty Acids
A 2025 randomized controlled trial evaluated omega-3-enriched lickable treats as adjunctive therapy in cats with FCGS. The study found that omega-3 supplementation was safe and associated with measurable improvements in clinical parameters compared to control, supporting a potential anti-inflammatory role for long-chain polyunsaturated fatty acids in this disease.18 Given the favorable safety profile of omega-3 supplementation, this is a reasonable adjunct to consider in cats that tolerate oral supplementation.
Vitamin D Supplementation Following Surgery
Cats with FCGS have been shown to have significantly lower serum vitamin D than healthy cats. A 2025 study evaluated post-operative vitamin D supplementation following mucogingival surgery in FCGS cats and found that supplementation significantly enhanced autophagy and improved quality of life measures.19 Given vitamin D’s known immunoregulatory role, this finding aligns with the broader understanding of immune dysfunction in FCGS and suggests that nutritional support may complement surgical and medical interventions.
Poly(styrene 4-sulfonate) (PSSNa)
A 2026 field study evaluated the antiviral effects of poly(styrene 4-sulfonate) (PSSNa), a sulfated polymer with known antiviral properties, in cats with FCV-associated oral infections.20PSSNa is thought to inhibit viral attachment and entry into host cells. While early-phase data, this work represents a growing interest in targeted antiviral strategies that specifically address FCV’s role in FCGS pathogenesis, complementing rather than replacing the immunomodulatory approaches that have dominated treatment to date.
Hypoallergenic Diet
A 2024 case report documented a cat with FCGS refractory to prednisolone, cyclosporine, and PME whose lesions resolved on a hypoallergenic diet.21 The lesions recurred upon return to the original diet and remitted again after reinstituting the elimination diet, providing a compelling clinical argument that food sensitivity may contribute to disease in at least a subset of cats. While this represents a single case, it has practical implications: for cats that remain refractory despite conventional interventions, a dietary trial with a novel protein or hydrolyzed diet is low-risk and potentially informative.
Lactoferrin
Oral bovine lactoferrin with and without an NSAID (piroxicam) has been explored as an adjunctive treatment for FCGS stomatitis.22,23. Lactoferrin has antimicrobial, antiviral, and immunomodulatory properties, and its oral delivery makes it a low-risk adjunct option.
Cannabidiol (CBD)
Interest in cannabidiol as an adjunctive therapy for FCGS has grown following two observations: first, that the oral mucosa of cats expresses cannabinoid and cannabinoid-related receptors, including CB1, CB2, and TRPV124; and second, that these receptors may play a role in local pain modulation and immune regulation in oral tissue.
A placebo-controlled trial of daily oral CBD as adjunctive treatment in cats with chronic gingivostomatitis found that CBD was well-tolerated and associated with modest improvements in clinical scores, though effect sizes were not dramatic.25 This remains a developing area, and CBD should currently be considered adjunctive rather than primary therapy.
Photobiomodulation and Photodynamic Therapy
Light-based therapies are attracting increasing attention in feline stomatitis. A 2024 case report described a refractory FCGS case that improved with topical indocyanine green (ICG)-mediated antimicrobial photodynamic therapy (aPDT) after failing conventional treatments including antibiotics, NSAIDs, and dental extraction.26 The antimicrobial and anti-inflammatory mechanisms of aPDT make it conceptually appealing in a disease driven in part by dysbiotic oral bacteria.
A 2024 study also assessed 830-nanometer low-level laser therapy (LLLT) in cats via extraoral application, finding preliminary evidence of biological effects that may be relevant to oral inflammation, though clinical application in FCGS remains early-stage.27
Several other therapies are used off-label or marketed for use for FCGS. Many of these therapies lack clinical trial data to demonstrate safety or efficacy for FCGS, and they are generally discouraged by the veterinary dental community for use in FCGS.
Putting It All Together: A Stepwise Approach
The evidence converges on a consistent stepwise framework for FCGS management:
- Step 1—Extraction first: PME or FME of diseased teeth and associated roots remains the primary intervention and should be pursued when diagnostically appropriate. Extraction helps remove the bacterial and viral burden. Without extraction, medical therapies may be less effective.
- Step 2—Adjunctive medical management:
- Pain management is crucial especially in cats that do not completely respond to extractions. Analgesic medications are also important during the post-surgical recovery from extractions and include gabapentin/pregabalin, amantadine, and buprenorphine. Options that do not require oral administration are preferred.
- Appetite support with an orexigenic therapy is often beneficial for cats that are losing weight or not eating well. There is a transdermal option to avoid oral medication for a cat with a painful mouth.
- Omega-3 supplementation, vitamin D (post-surgical), and dietary trials are low-risk measures that may add value alongside primary therapies
- Corticosteroids/Prednisolone can be used intermittently to manage flare-ups. Not recommended long term.
- Cyclosporine: consider in cats not improving post PME/FME if of low systemic risk for renal insufficiency, liver disease or diabetes mellitus. Monitor bloodwork routinely.
- Step 3–Cats that continue to have clinical signs and oral lesions 2 months following extractions and medical management are considered refractory and should be offered the next level of care rather than continuing palliative management alone. At this stage, consider adding IV mesenchymal stromal cell therapy (full description in Part 3: Understanding Stem Cell Therapy for Refractory. FCGS).
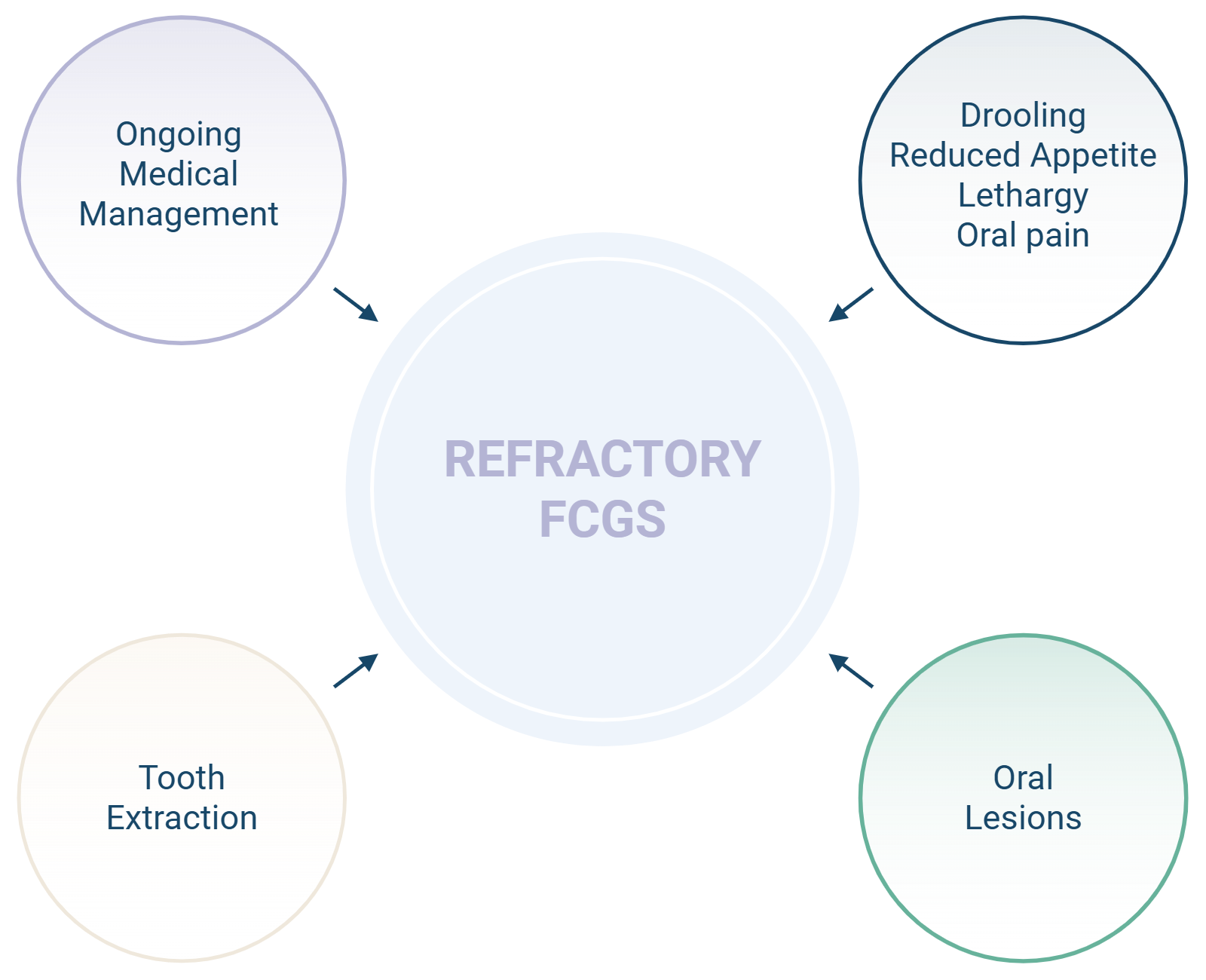
If your cat has had teeth extracted and is still not improving, please know that this is a recognized and documented occurrence—not a failure of care. Refractory FCGS is a well-described disease state, and there are additional options available. You are not out of options. Talk with your veterinarian about whether mesenchymal stromal cell (MSC) therapy might be the right next step for your cat. Gallant is currently enrolling for a clinical trial using Sonruvetcel, an IV MSC therapy for cats with refractory FCGS. Results from previous studies using Sonruvetcel demonstrated safety and efficacy in >75% cats at 90 days and continued improvement in 66% cats at 1 year.28,29
References
- Winer JN, Arzi B, Verstraete FJM. Therapeutic Management of Feline Chronic Gingivostomatitis: A Systematic Review of the Literature. Front Vet Sci. 2016;3. doi:10.3389/fvets.2016.00054
- Soltero-Rivera M, Goldschmidt S, Arzi B. Feline chronic gingivostomatitis: current concepts in clinical management. J Feline Med Surg. 2023;25(8):8. doi:10.1177/1098612X231186834
- Lobprise H, St Denis K, Anderson JG, Hoyer N, Fiani N, Yaroslav J. 2025 FelineVMA feline oral health and dental care guidelines. J Feline Med Surg. 2025;27(11):1098612X251398793. doi:10.1177/1098612X251398793
- Jennings MW, Lewis JR, Soltero-Rivera MM, Brown DC, Reiter AM. Effect of tooth extraction on stomatitis in cats: 95 cases (2000–2013). J Am Vet Med Assoc. 2015;246(6):6. doi:10.2460/javma.246.6.654
- Hussain Haidary M, Radzi R, Waseem Aslam M, Fong Lau S, Mustaffa Kamal F, Rasul Radzali A. Retrospective Study of Clinical Manifestations and Multiple Treatment Outcomes in 57 Cats Diagnosed with Feline Chronic Gingivostomatitis. J Anim Health Prod. 2021;10(1):1. doi:10.17582/journal.jahp/2022/10.1.51.59
- Silva M, Fernandes M, Fialho M, Mestrinho L. A Case Series Analysis of Dental Extractions’ Outcome in Cats with Chronic Gingivostomatitis Carrying Retroviral Disease. Animals. 2021;11(11):11. doi:10.3390/ani11113306
- Kim CG, Kwon D, Lee K, Kim SE, Jo HM. The prevalence of reasons for tooth extraction in cats. Front Vet Sci. 2025;12:1626701. doi:10.3389/fvets.2025.1626701
- Hennet PR, Camy GAL, McGahie DM, Albouy MV. Comparative efficacy of a recombinant feline interferon omega in refractory cases of calicivirus-positive cats with caudal stomatitis: A randomised, multi-centre, controlled, double-blind study in 39 cats. J Feline Med Surg. 2011;13(8):8. doi:10.1016/j.jfms.2011.05.012
- Lommer MJ. Efficacy of Cyclosporine for Chronic, Refractory Stomatitis in Cats: A Randomized, Placebo-Controlled, Double-Blinded Clinical Study. J Vet Dent. 2013;30(1):1. doi:10.1177/089875641303000101
- Choe KH, Jang K, Kim SE, Jo HM. Long-term efficacy of cyclosporine and interferon-ω in feline chronic gingivostomatitis: insights from SDAI scores. BMC Vet Res. 2025;21(1):708. doi:10.1186/s12917-025-05141-9
- Deleporte S, Briand A, Prélaud P. Ciclosporin oral solution in cats: a retrospective survey of compliance with treatment and adverse effects. J Feline Med Surg. 2024;26(2):1098612X231220848. doi:10.1177/1098612X231220848
- Rösch S, Frommeyer A, Schulte Bocholt J, Grote-Koska D, Brand K, Mischke R. Progression of cyclosporine A-blood levels in experimental cats receiving a high-dose treatment protocol. Front Vet Sci. 2024;11:1444586. doi:10.3389/fvets.2024.1444586
- Leal RO, Gil S. The Use of Recombinant Feline Interferon Omega Therapy as an Immune-Modulator in Cats Naturally Infected with Feline Immunodeficiency Virus: New Perspectives. Vet Sci. 2016;3(4):32. doi:10.3390/vetsci3040032
- Matsumoto H, Teshima T, Iizuka Y, et al. Evaluation of the efficacy of the subcutaneous low recombinant feline interferon-omega administration protocol for feline chronic gingivitis-stomatitis in feline calicivirus-positive cats. Res Vet Sci. 2018;121:53-58. doi:10.1016/j.rvsc.2018.10.003
- White C, Stavisky J. Does interferon‐ω treatment decrease clinical signs of feline chronic gingivostomatitis more rapidly than steroid treatment? Vet Rec. 2021;188(11):432-433. doi:10.1002/vetr.614
- White SD, Rosychuk RA, Janik TA, Denerolle P, Schultheiss P. Plasma cell stomatitis-pharyngitis in cats: 40 cases (1973-1991). J Am Vet Med Assoc. 1992;200(9):1377-1380.
- Tsang W, Linde A, Krumbeck JA, et al. Occurrence of Antimicrobial Resistance Genes in the Oral Cavity of Cats with Chronic Gingivostomatitis. Animals. 2021;11(12):3589. doi:10.3390/ani11123589
- Sukho P, Ploypetch S, Satthathum C, Prompiram P, Chakritbudsabong W. Efficacy and safety of omega-3-enriched lickable treats as adjunctive therapy for feline chronic gingivostomatitis: A randomized controlled trial. Vet World. Published online August 2025:2344-2356. doi:10.14202/vetworld.2025.2344-2356
- Huang YK, Chen CW, Renn TY, et al. Post-operative supplementation with vitamin D after mucogingival surgery significantly enhances autophagy and improves life quality following feline chronic gingivostomatitis. Int J Vet Sci Med. 2025;13(1):1-9. doi:10.1080/23144599.2025.2487751
- Synowiec A, Pachota M, Krejmer-Rabalska M, et al. Antiviral effect of poly(styrene 4-sulfonate) (PSSNa) on feline calicivirus oral infections in cats—field study. Vet Q. 2026;46(1):2616395. doi:10.1080/01652176.2026.2616395
- Silva LD, Martins T, Porsani MYH, Teixeira FA. The Impact of a Hypoallergenic Diet on the Control of Oral Lesions in Cats: A Case Report. Animals. 2024;14(18):18. doi:10.3390/ani14182656
- Hung YP, Yang YP, Wang HC, et al. Bovine lactoferrin and piroxicam as an adjunct treatment for lymphocytic-plasmacytic gingivitis stomatitis in cats. Vet J. 2014;202(1):76-82. doi:10.1016/j.tvjl.2014.06.006
- Sato R, Inanami O, Tanaka Y, Takase M, Naito Y. Oral administration of bovine lactoferrin for treatment of intractable stomatitis in feline immunodeficiency virus (FIV)-positive and FIV-negative cats. Am J Vet Res. 1996;57(10):10.
- Polidoro G, Galiazzo G, Giancola F, et al. Expression of cannabinoid and cannabinoid-related receptors in the oral mucosa of healthy cats and cats with chronic gingivostomatitis. J Feline Med Surg. 2021;23(8):679-691. doi:10.1177/1098612X20970510
- Coelho JC, Duarte N, Bento Da Silva A, Bronze MDR, Mestrinho LA. Placebo-Controlled Trial of Daily Oral Cannabidiol as Adjunctive Treatment for Cats with Chronic Gingivostomatitis. Animals. 2023;13(17):2716. doi:10.3390/ani13172716
- Hou CJ, Chen TY, Wong TW. Topical indocyanine green antimicrobial photodynamic therapy for refractory feline chronic gingivostomatitis: A case report. Photodiagnosis Photodyn Ther. 2024;50:104373. doi:10.1016/j.pdpdt.2024.104373
- Kamlangchai P, Kampa N, Srithunyarat T, et al. Assessing the potential efficacy of 830-nanometer low-level laser therapy in cats: Extraoral applications. Vet World. Published online May 2024:1124-1129. doi:10.14202/vetworld.2024.1124-1129
- Williams V, Schneider JL, Parrish RS, et al. EXPRESS: Clinical field study evaluating the safety and efficacy of allogeneic uterine-derived mesenchymal stem cells for refractory feline chronic gingivostomatitis (FCGS). J Feline Med Surg. Published online September 25, 2025:1098612X251385852. doi:10.1177/1098612X251385852
- Williams V, Schneider JL, Parrish RS, et al. EXPRESS: A long-term field safety study evaluating allogeneic uterine-derived mesenchymal stem cells for refractory feline chronic gingivostomatitis (FCGS). J Feline Med Surg. Published online February 27, 2026:1098612X261431058. doi:10.1177/1098612X261431058

Vice President of Veterinary Affairs at Gallant
Dr. Rebecca Windsor, DVM, DACVIM, is a board-certified veterinary neurologist with over 20 years of clinical experience and a strong record of scientific publication. She joined Gallant in 2025 and serves as Vice President of Veterinary Affairs.
Dr. Windsor specializes in veterinary regenerative medicine, with a focus on advancing FDA-approved, off-the-shelf mesenchymal stem cell therapies for pets. She develops educational platforms that translate the science, safety, and clinical efficacy of stem cell therapy for veterinary professionals. Since 2019, she has served as a Clinician Scientist at Ethos Discovery, where she leads the neurology research portfolio.


