FCGS Educational Series Part 3: Understanding Mesenchymal Stromal Cell (MSC) Therapy for Refractory FCGS
This is Part 3 of our three-part Educational Series on Feline Chronic Gingivostomatitis (FCGS).
- Read Part 1: What Causes FCGS? Understanding the Roots of a Debilitating Disease
- Read Part 2: Managing FCGS—Historical Treatment Approaches
For cats with refractory feline chronic gingivostomatitis (rFCGS), the emergence of mesenchymal stromal/stem cell (MSC) therapy represents a potential first treatment that targets the underlying immune dysregulation while also controlling clinical signs. But how do these cells work, and how strong is the evidence behind them?
- MSCs regulate the overall immune system dysregulation.
- MSCs also have anti-inflammatory and pain-relieving properties through cell-to-cell signaling and cytokine regulation.
- MSC therapy has been studied in refractory FCGS (rFCGS) cats who remain symptomatic after tooth extraction and ongoing medical management.
- Clinical studies with uterine-derived MSCs have shown improvement in quality-of-life measurements.
- Improvements in how a cat feels often occur before visible healing in the mouth.
In Part 1 of this series, What CausesFCGS? Understanding the Roots of a Debilitating Disease, we covered what FCGS is and why so many cats remain refractory. In Part 2, Managing FCGS — Traditional Treatment Approaches, we reviewed the evidence behind traditional therapies for FCGS. Now in Part 3, we turn our focus to MSC therapy for refractory FCGS. We examine the evidence in depth, exploring how MSC therapy targets the disease at its source, as well as the safety and efficacy data supporting its use in this challenging condition.
Why Standard Treatments May Fall Short
FCGS is not simply a disease of the mouth. It is a systemic immune-mediated condition driven by abnormal T-cell activation, dysregulated oral microbiome, and viral triggers, particularly feline calicivirus (FCV), which is detected in approximately 60–90% of affected cats.1,2
Dental extraction removes the plaque-coated teeth that amplify this antigenic burden, and although extraction alone works for many cats, approximately 1/3 of cats remain refractory after partial or full-mouth extractions,3,4 often requiring lifelong immunosuppressive medications. These medications blunt inflammation but do not address the underlying immune imbalance. Disease typically recurs when drugs are withdrawn, and long-term use carries some toxicity risks.5
Critically, systemic markers of inflammation including elevated neutrophils and globulins, altered T-cell ratios, and elevated inflammatory cytokines persist even after extractions, underscoring that the disease may not always be fully managed through traditional therapies alone.6,7 It is this broader immune dysregulation that MSC therapy is designed to address.
In simple terms, MSC therapy works by recalibrating the cat’s overactive immune response at its source, whereas immunosuppressive medications dampen immune activity broadly and temporarily, requiring continuous dosing without addressing the underlying immune dysregulation driving FCGS.
What Are MSCs?
MSCs are present in connective tissues throughout the adult body, and common sources for MSC therapies include fat, bone marrow, and the uterus. These differ from embryonic or other non-adult sourced stem cells. Rather than engrafting and differentiating permanently into new tissue, their primary role is to rebalance the immune system by releasing factors that influence host tissue cells and immune cells throughout the blood and diseased tissue, thereby reducing inflammation and promoting tissue repair in a natural way.8,9 In FCGS, it is precisely these immunomodulatory properties that inherently allow the cells to directly address the chronic immune dysregulation. Some cats with FCGS have concurrent bacterial or viral infection, and while MSCs don’t kill pathogens directly, they help the immune system mount a more balanced and effective response to clear them.
MSCs do not simply suppress the immune system. Instead, they help balance immune cell activity, dampening overactive pathways while simultaneously enhancing the immune system’s ability to fight viral infection. This dual capacity makes them uniquely suited to rFCGS, which involves both hyperimmune inflammation and a defective antiviral response.
Mechanisms of Action in rFCGS:
The sections below describe how MSCs work at a cellular level. While detailed, they help explain why this therapy may behave differently from traditional treatments.
1. T-Cell Immunomodulation
T cells are specialized immune cells that patrol the oral tissues of cats, defending against pathogens while tolerating normal oral bacteria and dietary antigens to maintain mucosal health. The immunopathology of FCGS is defined by T-cell dysregulation: a systemic expansion of CD8+ effector memory T cells, a reduced CD4/CD8 ratio, and excessive lymphocyte proliferation that perpetuates mucosal destruction.10 MSCs have been shown to directly suppress this abnormal T-cell activity through multiple mechanisms.
MSCs interact with T cells via adhesion molecules — specifically ICAM-1/LFA — and through secretion of prostaglandin E2 (PGE2), which induces cell-cycle arrest in mitogen-activated lymphocytes during the G0 and G1 phases of mitosis, reducing peripheral blood mononuclear cell (PBMC) proliferation.11
Clinical studies in cats with rFCGS have confirmed these effects in vivo: following MSC administration, treated cats demonstrated significant decreases in circulating neutrophils, reductions in IFN-γ and IL-1β, decreases in the quantity of circulating cytotoxic T cells, and normalization of CD4/CD8 ratios.6
Key takeaway: MSCs have been shown to reduce cells and factors that promote inflammation, ulceration, and pain inside the mouth of cats with FCGS establishing, an environment conducive to healing of oral lesions.
2. Enhancement of Antiviral CD8+ Cytotoxic Function
Importantly, while MSCs suppress abnormal T-cell proliferation, they simultaneously enhance the functional cytotoxic capacity of CD8+ T cells — which is precisely what is needed to combat the infectious drivers of FCGS.
MSCs alter the phenotypic and functional characteristics of CD8+ T cells, upregulating effector compounds including granzyme B, IL-2, and the killer cell lectin-like receptor subfamily G1 (KLRG-1).13 Co-culture of MSCs with T cells reduces CD8 and CD62L expression while upregulating CD57 and CD25,11 shifting CD8+ cells toward a more potent terminally differentiated effector phenotype better able to eliminate virally infected cells.14
Medications such as corticosteroids and cyclosporine cause global immunosuppression but have no influence on antiviral immunity, highlighting a critical mechanistic advantage of MSCs over immunosuppressants in FCGS.
Key takeaway: MSCs have been shown to enhance the ability of immune cells to clear viral infection.
3. Direct Antiviral Properties
MSCs appears to act on the viral component of FCGS beyond just improving immune surveillance. The secretome of MSCs has been shown to prevent replication of both FCV and feline herpesvirus type 1 (FHV1) in vitro, though without blocking viral entry into cells.15,16 This antiviral secretome activity may contribute to the healing of oral lesions observed in clinical responders.
Key takeaway: MSCs have been shown to reduce the replication of viruses inside cells, thereby lowering the overall viral burden inside the cells.
4. Cytokine and Inflammatory Mediator Normalization
The inflammatory cytokine profile in FCGS is substantially elevated. Transcriptomic analyses show overexpression of IL-1β, IL-2, IL-4, IL-6, IL-10, IL-12, TNF-α, IFN-γ, and notably IL-17A — the signature cytokine of Th17 cells, which are implicated in both mucosal destruction and bone loss.7,18 MSC administration reduces systemic IFN-γ and IL-1β levels,6 downregulating the inflammatory cascade that drives chronic oral mucosal damage.
Key takeaway: MSCs have been shown to reduce inflammatory markers in the bloodstream as well as in the tissues.
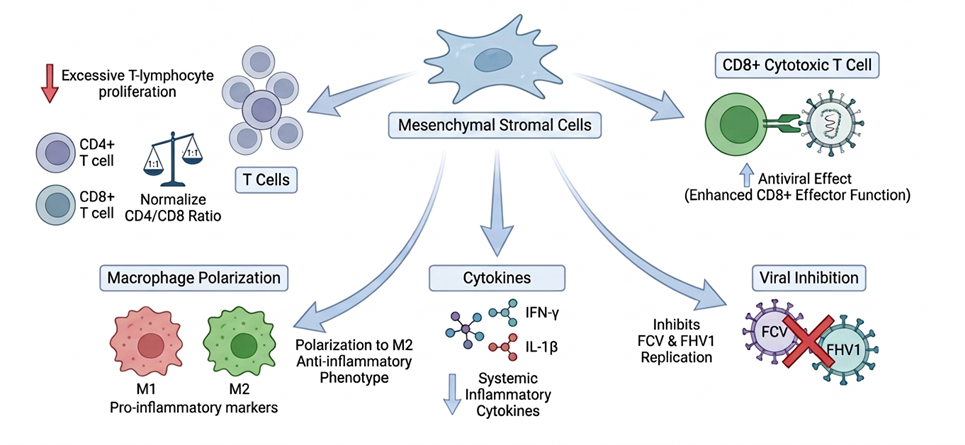
- Inhibit excessive T-lymphocyte proliferation
- Normalize CD4/CD8 T-cell ratios
- Enhance CD8+ cytotoxic T cell antiviral effector function
- Polarize macrophages toward anti-inflammatory M2 phenotype
- Inhibit FCV and FHV1 replication
The Clinical Evidence: What This Means for Cats
While the science behind MSC therapy is complex, clinical studies focus on what matters most: whether cats feel better. Many cat parents report improvements in comfort, appetite, and social interaction before visible healing in the mouth is seen during a veterinary exam.
Adipose-Derived MSCs
The first clinical trials using MSC therapy for rFCGS were conducted at the University of California, Davis, using fresh autologous (cells sourced from the same animal) and allogeneic (cells sourced from a different animal of the same species) feline adipose-derived MSCs (A-MSCs). Cats received two intravenous doses of 20 million cells approximately 30 days apart, with each serving as its own control given the refractory nature of disease.
Initial results showed marked improvement or complete resolution in 57-70% of cats treated with autologous or allogeneic MSCs.6,19 There was no statistically significant difference between autologous and allogeneic response rates, a finding that has positive practical implications, since allogeneic cells are far more accessible and scalable than autologous harvesting from each patient.20
Long-Term Outcomes: Nine Years of Follow-Up
The longest follow-up study of MSC therapy for rFCGS followed 38 client-owned cats for 2 to 9 years after treatment.20 The findings support MSC therapy as a durable intervention:
| 65.5% Overall positive response rate at long-term follow-up | 58.6% Permanent improvement or cure (36–108 months) |
| 83% Mean reduction in lesion score at recheck | 90.6% Clients willing to pursue MSC therapy again |
One clinical finding from this study was that a cat’s response status at 6 months post-treatment was positive predictor of long-term outcome21, however clinical success is still possible in some cats past the 6-month window as healing occurs at variable rates.
While adipose-derived MSCs showed therapeutic promise, their practical availability is limited and a single harvest from a patient may not result in an adequate number of viable cells. Harvesting autologous adipose MSCs requires an invasive surgical procedure in an already ill patient, and autologous expansion can be complicated by feline foamy virus (FFV), which is present in approximately 50–55% of adipose-derived MSC lines from client-owned cats and causes cellular senescence and renders cells unsuitable for infusion.21 Use of allogeneic cells allows for screening of feline foamy virus in the donor (testing commercially unavailable). In addition to demonstrating safety and efficacy of allogeneic MSCs for rFCGS, the UC Davis studies highlighted the need for a donor-derived, ready-to-use on-demand option for cats with rFCGS.
Uterine-Derived MSCs – Ready-to-Use On-Demand MSC Therapy for Cats with rFCGS
Gallant’s MSCs are uterine-derived (UMSCs) collected from FDA qualified, healthy, specific pathogen-free feline donors collected during routine spay surgeries. The therapy is manufactured under Good Manufacturing Practice (GMP) conditions and regulated as an FDA drug. Sonruvetcel is under investigational use as a potential ready-to-use, off-the-shelf product with verified sterility, stability, purity, dose and potency.
Efficacy Outcomes
The largest clinical trial of MSC therapy for rFCGS to date was completed and published in 2025 by Gallant’s researchers. The study was conducted to support reasonable expectation of effectiveness for FDA approval and was a 90-day prospective, multi-site, baseline-controlled clinical field trial involving 46 cats across nine veterinary dental specialty hospitals across the United States.21 Cats received two intravenous doses of 20 million UMSCs 14 days apart.
The results demonstrated clinically relevant improvements across multiple outcome measures:
| 78.8% Improved quality of life based on Client Specific Outcome Measures (CSOM) at Day 90 | 75.8% Mildly or greatly improved caregiver overall response rate at Day 90 |
| 52.3% Improvement in quality of life after the first dose at Day 14 | 45.5% Improvement of at least 25% in veterinary assessed oral lesion score at Day 90 |
More than half of cats showed measurable quality-of-life improvement within 14 days, before receiving the second dose. This early improvement in clinical signs and quality of life is consistent with the proposed systemic immunomodulatory mechanism of action, wherein UMSCs normalize the broader immune dysregulation of FCGS before oral mucosal healing becomes visible.22
For cat parents, these early changes are often seen as improvements in appetite, comfort, and interaction before visible healing in the mouth.
Cats treated within 6 months of dental extraction showed greater improvement in clinical outcomes, supporting earlier intervention in the post-extraction window.22
Safety outcomes:
Adverse events (defined as any untoward medical occurrence associated with the use of a drug, whether or not considered drug related) were predominantly mild and transient. There were no serious AEs reported in the study associated with treatment administration. The non-serious adverse events reported associated with treatment (within 24 hours) are shown below with nausea and vomiting being the most common in 15.2% of the cats treated. There are no expected AEs beyond 24 hours following treatment.
Non-serious adverse events reported within 24 hours of treatment
| Adverse Reaction | Number of Cats |
| Vomiting/Nausea | 7 |
| Tachypnea | 3† |
| Diarrhea | 3 |
| Hypersalivation | 2 |
| Pyrexia | 2‡ |
| Dyspnea | 1 |
‡ One cat had pyrexia associated with injection on both administration days; a second cat had pyrexia on one of the two administration days.
There were six serious adverse events during the study; all were reported by investigators to be unrelated to UMSC administration. Routine hematology, biochemistry, and urinalysis showed no consistent, clinically relevant trends over the 90-day period.22
One-Year Efficacy and Safety Follow-Up:
The long-term safety study published by Gallant researchers in 2026 followed 35 of the original 46 cats through Day 365, providing the first prospectively collected one-year safety and effectiveness data for MSC therapy in cats with rFCGS.23 In this study, cats were allowed to resume immunosuppressant and immunomodulatory medications as needed that were withdrawn for the first 90 days of the study.
66% of cats did not restart medical therapy after UMSC treatment, and of those that did restart, 75% used medications only short term for flare ups. Only 8.6% of cats required an ongoing immunosuppressant.
| Timepoint | Key Outcomes |
| Day 90 (end of primary study) | 76% of cats showed significant caregiver overall improvement 46% of cats showed significant oral lesion improvement |
| Day 180 (6 months) | 76% of cats showed significant caregiver overall improvement 52% of cats showed significant oral lesion improvement |
| Day 270 (9 months) | 66% of cats showed significant caregiver overall improvement 50% of cats showed significant oral lesion improvement |
| Day 365 (1 year) | 66% of cats showed significant caregiver overall improvement 47% of cats showed significant oral lesion improvement 22% of cats achieved complete clinical cure 69% of cats gained weight |
69% of cats gained weight over the year, with a mean increase of 16.2% — a meaningful quality-of-life marker in cats whose pre-treatment disease had caused chronic anorexia and weight loss.23 No immunogenic or tumorigenic safety concerns emerged over the full year of follow-up.
Efficacy Duration
One of the most consistent findings across all MSC studies for rFCGS is that quality-of-life improvement precedes visible oral lesion healing — often by months. Cat parents report increases in appetite, grooming behaviors, play and activity, social interaction, and reduction in pain behaviors within hours to days of infusion, while veterinarian-assessed mucosal lesion scores improve more slowly, sometimes requiring 6–18 months for full resolution.23,23,19
This temporal pattern is mechanistically coherent. The rapid systemic immunomodulatory effects of MSCs — T-cell rebalancing, cytokine normalization, and macrophage repolarization — improve the cat’s systemic inflammatory burden quickly. There are likely other mechanisms in addition to a reduction in inflammation that impact clinical improvement. Mucosal healing, by contrast, requires sustained immune normalization and tissue remodeling/healing which requires time (months). The time to maximal lesion improvement in cats that respond to treatment varies. Cure (no oral lesions) has been observed as early as 90 days in some cats. It is therefore important that clinicians and cat parents understand that absence of rapid mucosal healing does not indicate treatment failure.
The difference between how a cat feels and what is visible on exam is an important part of understanding how MSC therapy works and setting expectations for response to treatment.
Timing of MSC Therapy
One small clinical study demonstrated that MSC therapy administered prior to full-mouth extraction showed no substantial clinical benefit24, suggesting extraction should come first to remove the persistent antigenic stimulus. MSCs can then address the residual immune dysregulation that extraction alone may not resolve. Future studies in a larger number of cats are necessary to continue to evaluate the use of MSC therapy before or at the time of extraction.
Emerging evidence also suggests that earlier treatment post extraction plays a potential role in maximizing potential response to treatment. Cats treated within 6 months of extraction showed better oral lesion response in the 2025 Gallant trial,22 and it is plausible that administering MSCs closer to the post-extraction window may improve outcomes further.
The Broader Picture: Where MSC Therapy Fits
Collective review of the literature for adipose-derived, placental-derived, and uterine-derived MSCs in cats with refractory FCGS supports that intravenous MSC therapy is well tolerated and may be effective in achieving remission or alleviating the clinical signs of rFCGS in cats that have undergone dental extraction.25 The overall success of MSC therapy has been estimated to increase the overall rate of FCGS remission from roughly 70% to approximately 90%.20 Gallant studies support that approximately 75% of cats will experience clinically meaningful improvement in quality of life with UMSC treatment by 3 months regardless of the time to improvement in oral lesions. Gallant studies also support that approximately 22% of cats will achieve remission (healing of oral lesions) by one year following treatment.
Uterine-derived allogeneic MSCs represent the next generation of therapy for cats with refractory FCGS — manufactured to pharmaceutical standards under FDA guidance as a ready-to-use, off-the-shelf product. Gallant’s data supports the safety and efficacy for cats suffering from this debilitating disease.
As research continues, MSC therapy represents an evolving area of feline medicine focused on addressing immune-driven disease at its source.
References
- Sánchez-Vallejo M, Vélez-Velásquez P, Correa-Valencia NM. Feline chronic gingivostomatitis: a thorough systematic review of associated factors. J Feline Med Surg. 2025;27(4):1098612X241310590. doi:10.1177/1098612X241310590
- Fried WA, Soltero-Rivera M, Ramesh A, et al. Use of unbiased metagenomic and transcriptomic analyses to investigate the association between feline calicivirus and feline chronic gingivostomatitis. Am J Vet Res. 2021;82(5):381–394. doi:10.2460/ajvr.82.5.381
- Jennings MW, Lewis JR, Soltero-Rivera MM, Brown DC, Reiter AM. Effect of tooth extraction on stomatitis in cats: 95 cases (2000–2013). JAVMA. 2015;246(6):654–660. doi:10.2460/javma.246.6.654
- Lee DB, Verstraete FJM, Arzi B. An update on feline chronic gingivostomatitis. Vet Clin North Am Small Anim Pract. 2020;50(5):973–982. doi:10.1016/j.cvsm.2020.04.002
- Winer JN, Arzi B, Verstraete FJM. Therapeutic management of feline chronic gingivostomatitis: a systematic review. Front Vet Sci. 2016;3:54. doi:10.3389/fvets.2016.00054
- Arzi B, Mills-Ko E, Verstraete FJM, et al. Therapeutic efficacy of fresh, autologous mesenchymal stem cells for severe refractory gingivostomatitis in cats. Stem Cells Transl Med. 2016;5(1):75–86. doi:10.5966/sctm.2015-0127
- Peralta S, Grenier JK, Webb SM, et al. Transcriptomic signatures of feline chronic gingivostomatitis are influenced by upregulated IL6. Sci Rep. 2023;13(1):13437. doi:10.1038/s41598-023-40679-4
- von Bahr L, Batsis I, Moll G, et al. Analysis of tissues following mesenchymal stromal cell therapy in humans indicates limited long-term engraftment. Stem Cells. 2012;30:1575–1578.
- Luger D, Lipinski MJ, Westman PC, et al. Intravenously delivered mesenchymal stem cells: systemic anti-inflammatory effects. Circ Res. 2017;120:1598–1613.
- Vapniarsky N, Simpson DL, Arzi B, et al. Histological, immunological, and genetic analysis of feline chronic gingivostomatitis. Front Vet Sci. 2020;7:310. doi:10.3389/fvets.2020.00310
- Taechangam N, Iyer SS, Walker NJ, Arzi B, Borjesson DL. Mechanisms utilized by feline adipose-derived mesenchymal stem cells to inhibit T lymphocyte proliferation. Stem Cell Res Ther. 2019;10(1):188. doi:10.1186/s13287-019-1300-3
- Park SG, An JH, Li Q, et al. Feline adipose tissue-derived mesenchymal stem cells pretreated with IFN-γ enhance immunomodulatory effects through the PGE2 pathway. J Vet Sci. 2021;22(2):e16. doi:10.4142/jvs.2021.22.e16
- Taechangam N, Walker NJ, Borjesson DL. Feline adipose-derived mesenchymal stem cells induce effector phenotype and enhance cytolytic function of CD8+ T cells. Stem Cell Res Ther. 2021;12(1):495. doi:10.1186/s13287-021-02558-5
- Rivas IL, Soltero-Rivera M, Vapniarsky N, Arzi B. Stromal cell therapy in cats with feline chronic gingivostomatitis: current perspectives and future direction. J Feline Med Surg. 2023;25(8):1098612X231185395. doi:10.1177/1098612X231185395
- Teshima T, Yasumura Y, Suzuki R, Matsumoto H. Antiviral effects of adipose tissue-derived MSC secretome against feline calicivirus and FHV1. Viruses. 2022;14(8):1687. doi:10.3390/v14081687
- Taechangam N. Pilot Efficacy of Allogeneic Uterine-Derived Mesenchymal Stromal Cells for the Treatment of Refractory Feline Chronic Gingivostomatitis (FCGS). NAVMRA Proceedings. Published online 2023.
- Weber MG, Walters-Laird CJ, Kol A, et al. Gut germinal center regeneration and enhanced antiviral immunity by MSCs in SIV infection. JCI Insight. 2021;6:e149033. doi:10.1172/jci.insight.149033
- Soltero-Rivera M, Shaw C, Arzi B, Lommer M, Weimer B. Feline chronic gingivostomatitis diagnosis and treatment through transcriptomic insights. Pathogens. 2024;13(3):192. doi:10.3390/pathogens13030192
- Arzi B, Clark KC, Sundaram A, et al. Therapeutic efficacy of fresh, allogeneic mesenchymal stem cells for severe refractory feline chronic gingivostomatitis. Stem Cells Transl Med. 2017;6(8):1710–1722. doi:10.1002/sctm.17-0035
- Soltero-Rivera M, Hart S, Blandino A, Vapniarsky N, Arzi B. Mesenchymal stromal cell therapy for feline chronic gingivostomatitis: long term experience. Front Vet Sci. 2023;10:1171922. doi:10.3389/fvets.2023.1171922
- Arzi B, Kol A, Murphy B, et al. Feline foamy virus adversely affects feline mesenchymal stem cell culture and expansion. Stem Cells Dev. 2015;24(7):814–823. doi:10.1089/scd.2014.0317
- Williams VS, Schneider JL, Parrish RS, et al. Clinical field study evaluating the safety and efficacy of allogeneic uterine-derived mesenchymal stem cells for refractory feline chronic gingivostomatitis. J Feline Med Surg. 2025. doi:10.1177/1098612X251385852
- Williams VS, Schneider JL, Parrish RS, et al. A long-term field safety study evaluating allogeneic uterine-derived mesenchymal stem cells for refractory feline chronic gingivostomatitis. J Feline Med Surg. 2026 (Author Accepted Manuscript). doi:10.1177/1098612X261431058
- Arzi B, Taechangam N, Lommer MJ, Walker NJ, Loscar MR, Borjesson DL. Stem cell therapy prior to full-mouth tooth extraction lacks substantial clinical efficacy in cats with FCGS. J Feline Med Surg. 2021;23(6):604–608. doi:10.1177/1098612X20967172 Nekouei O, Tung Wong S, Ka Yi Leung T, et al. Effectiveness of mesenchymal stem cell therapy in cats with chronic gingivostomatitis. VE. 2024;9(1). doi:10.18849/ve.v9i1.680

Vice President of Veterinary Affairs at Gallant
Dr. Rebecca Windsor, DVM, DACVIM, is a board-certified veterinary neurologist with over 20 years of clinical experience and a strong record of scientific publication. She joined Gallant in 2025 and serves as Vice President of Veterinary Affairs.
Dr. Windsor specializes in veterinary regenerative medicine, with a focus on advancing FDA-approved, off-the-shelf mesenchymal stem cell therapies for pets. She develops educational platforms that translate the science, safety, and clinical efficacy of stem cell therapy for veterinary professionals. Since 2019, she has served as a Clinician Scientist at Ethos Discovery, where she leads the neurology research portfolio.


