Feline Osteoarthritis Series Part 1: What Causes Osteoarthritis?
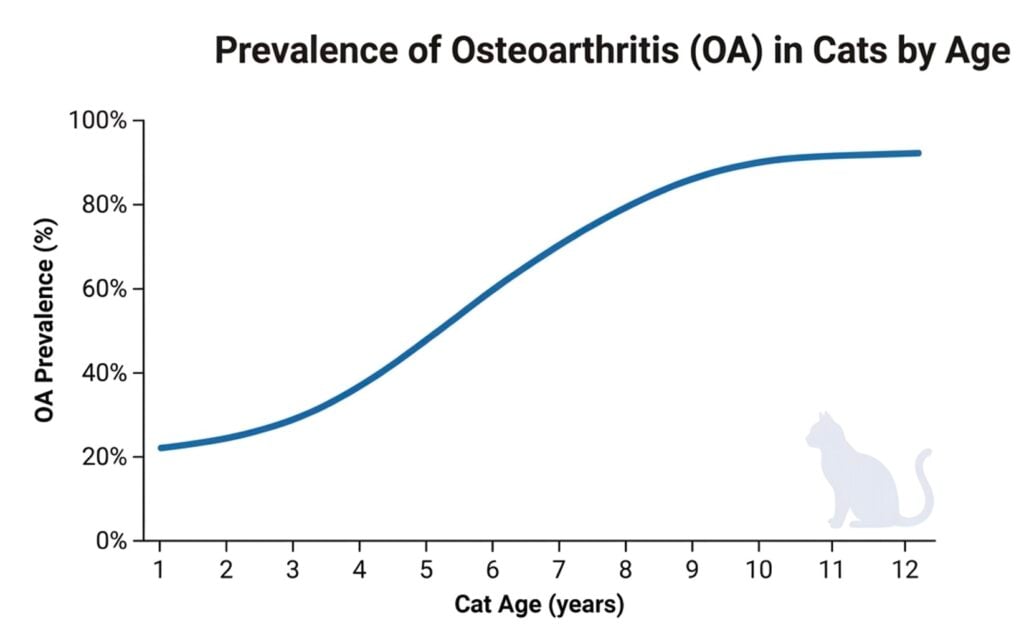
Osteoarthritis (OA), also termed degenerative joint disease (DJD) in the feline literature, is now recognized as one of the most common and underdiagnosed chronic conditions of domestic cats. Depending on the population studied and the diagnostic threshold used, radiographic OA has been reported to range from 22% to greater than 90% of cats, with 61% of cats over 6 years of age3 and 91–92% of geriatric cats showing evidence of OA 1–5. For decades, feline OA was framed as either a rare orthopedic condition or an unavoidable consequence of aging; however, that framing is outdated. Contemporary research portrays feline OA as a complex, whole-joint disease in which mechanical, inflammatory, metabolic, immunologic, and neurobiological processes converge to drive progressive structural failure of the osteochondral unit and chronic pain that markedly compromises quality of life6–8. Understanding this revised model matters clinically, because to a greater degree than in dogs, clinical signs of feline OA are subtle, bilateral, and easily mistaken for “normal” aging.
Why “Wear and Tear” Doesn’t Tell the Whole Story in the Cat
A strong argument has been made that feline OA development is heavily influenced by cumulative chronic repetitive microtrauma over a cat’s lifespan. Feline OA is highly prevalent, frequently bilateral and symmetrical5,9, and most commonly affects the elbow, hip, stifle, tarsus, and shoulder3–5. However, age and mechanical wear alone do not fully explain how or where feline osteoarthritis (OA) develops. Unlike dogs, cats are much less likely to develop OA secondary to hip dysplasia or other developmental joint disorders. In cats, the effects of joint injury appear to be amplified by a systemic, multifocal disease process, with immunologic and immunometabolic dysfunction playing a major role in disease progression.
Articular cartilage in cats, as in other mammals, is composed primarily of water, type II collagen, and proteoglycans, with chondrocytes representing only a small fraction of tissue volume. Histological and molecular work in feline humeral condylar OA has demonstrated that affected cartilage shows altered expression of matrix and matrix-modifying genes, consistent with active remodeling rather than passive erosion10. The repair response in feline cartilage, as in other species, typically yields biomechanically inferior fibrocartilage. This biological reality means that feline joints, despite their normally smaller load, have little tolerance for the cycle of microdamage and aborted repair that defines OA.
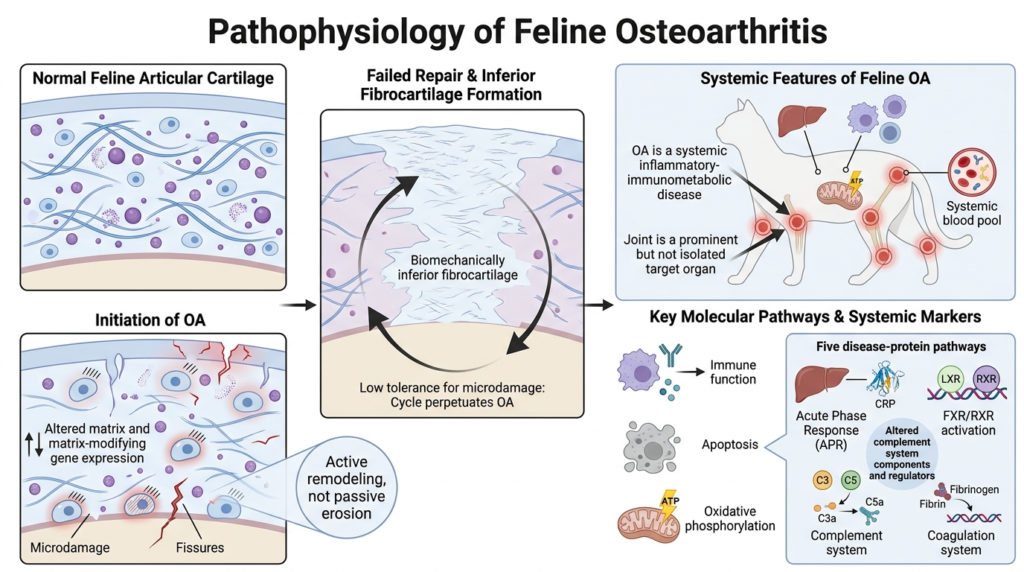
Recent genomic and proteomic work has reframed feline OA as a systemic, not merely articular, condition. Differential gene expression has been identified in cats with OA, strongest in three biological pathways: immune function, apoptosis, and oxidative phosphorylation11. Serum proteomic profiles in OA cats show alterations in complement system components and regulators11. Together, these findings reposition feline OA as a whole-body inflammatory-immunometabolic disorder in which the joint is a prominent (but not isolated) target organ.
A study evaluating serum protein analysis in cats with varying degrees of CKD, OA, and pain with documented radiographs and pain assessment in each joint allowed pathway analysis to be anchored to disease burden rather than presence/absence alone12. Five pathways emerged as dominant in the OA + pain disease state: acute phase response (APR) signaling, liver X receptor (LXR)/retinoid X receptor (RXR) activation, farnesoid X receptor (FXR)/RXR activation, the complement system, and the coagulation system12. Notably, the liver (through hepatocyte-derived acute phase proteins, lipid-metabolism regulators, and complement components) emerges as a previously underappreciated regulatory organ in the systemic biology of feline DJD, linking joint pathology, chronic pain, and chronic relative low-grade inflammation12.
The Mechanical-Inflammatory Loop: How Feline OA Actually Develops
Feline OA, like canine and human OA, can be productively understood as the outcome of either abnormal forces acting on a normal joint, or normal forces acting on an abnormal joint. Once an inciting event occurs, a self-amplifying loop of mechanical and inflammatory signaling ensues.
Synovial Inflammation, Cytokines, and Cartilage Catabolism
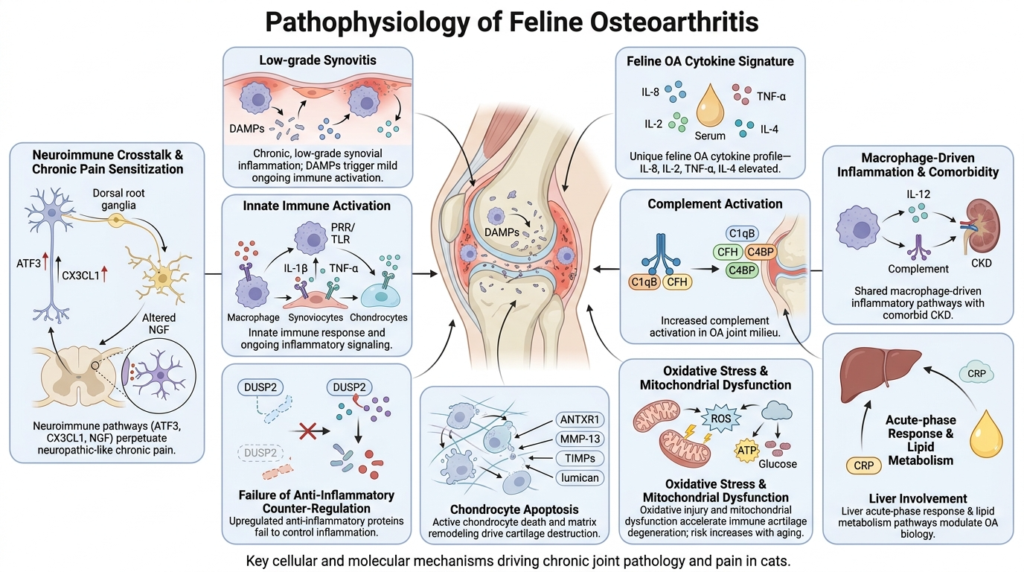
Cartilage breakdown products released into the synovial fluid act as damage-associated molecular patterns (DAMPs), which are scavenged by synovial macrophages, initiating synovitis. Activated synoviocytes and chondrocytes secrete pro-inflammatory cytokines—most importantly interleukin-1β (IL-1β) and tumor necrosis factor-α (TNF-α)—which in turn upregulate matrix metalloproteinases (MMPs), nitric oxide, and reactive oxygen species. Although feline-specific data remain sparse compared with other species, a gene expression study in the feline humeral condyle confirmed cat-specific upregulation of cartilage matrix–degrading and remodeling genes in OA tissue10.
One study using feline-specific cytokine data demonstrated that cats with higher radiographic DJD scores had higher serum concentrations of IL-4 and IL-8, while cats with higher orthopedic pain scores had higher concentrations of IL-8, IL-2, and TNF-α14. Notably, no single cytokine or panel reliably discriminated DJD cats from controls—a reminder that serum cytokine signatures in feline OA are present but complex. The increase in IL-8 was at least partially confounded by age, since DJD cats in the cohort were also older than controls14. The cytokine signature of feline DJD does not map cleanly onto either human or canine OA, and age and disease are difficult to separate in the cat.
One protein analysis study identified upregulation in a receptor that triggers chondrocyte apoptosis and matrix mineralization in cats with OA, consistent with chondrocyte apoptosis as a causative event in cartilage failure12. Cartilage acidic protein 1 (CRTAC1), induced in chondrocytes and synovial fibroblasts by pro-inflammatory cytokines and previously identified as a pain-correlated biomarker in human knee OA, was specifically upregulated in cats with higher pain scores12. Complement components and regulators were among the differentially abundant proteins common to cats with DJD and pain, further supporting a complement-mediated pathobiology now established in human OA12. Several proteins with homeostatic or anti-inflammatory roles were also upregulated including dual specificity phosphatase 2 (DUSP2), which suppresses IL-1β–induced chondrocyte inflammation, consistent with a compensatory but potentially insufficient counter-regulatory response12.
The Neurobiological Signature of Feline OA Pain
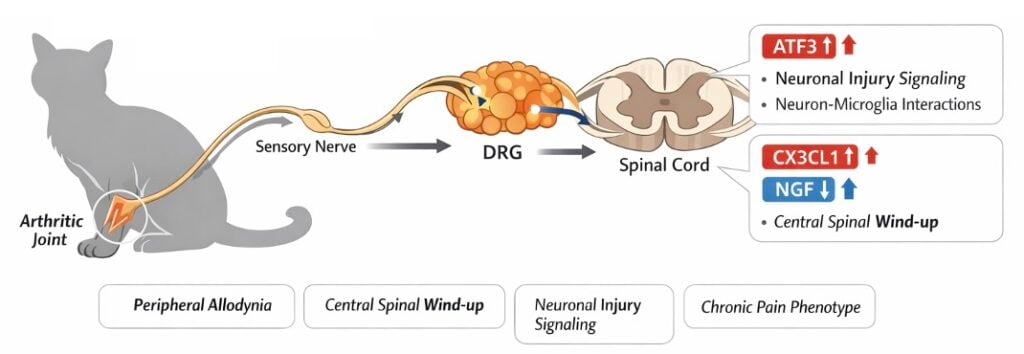
Feline OA is also associated with chronic pain with measurable changes in the peripheral and central nervous systems. Sensory testing in cats with naturally occurring OA pain has demonstrated both central sensitization (neurons in the spinal cord and brain become increasingly responsive, resulting in an exaggerated perception of pain) with allodynia (pain in response to a stimulus that would not normally be painful) 15,16. These clinical findings have been characterized at the molecular level in feline tissue. A study examining lumbar dorsal root ganglia (DRG) and dorsal horn spinal cord from cats with naturally occurring OA-associated pain compared with healthy controls demonstrated upregulation of activating transcription factor 3 (ATF3) and fractalkine (CX3CL1) in DRG of DJD cats, and upregulation of CX3CL1 with concurrent downregulation of nerve growth factor (NGF) in the spinal cord17. These changes are consistent with a chronic pain phenotype involving neuronal injury markers (ATF3), neuron–microglia signaling (CX3CL1) and altered neurotrophin biology (NGF).
Subchondral Bone: An Underappreciated Driver in the Cat
The subchondral bone is an active participant in feline OA. In feline humeral condylar OA, molecular analysis has shown coordinated changes in cartilage-derived and bone-derived matrix proteins, suggesting disease is not just localized to the cartilage10. Radiographic features classically described in feline OA including osteophytosis (often mild compared with the dog), subchondral sclerosis, intra-articular mineralization, and enthesophytosis exemplify this pathological bony change1,3,9. Importantly, osteophyte formation in cats tends to be less prolific than in dogs—one reason why feline radiographic OA was historically under-recognized and why orthopedic examination and owner-reported behavior with validated metrology instruments are essential adjuncts to imaging3,7,9. It is important as clinicians that we do not judge the need for intervention based solely on radiographs.
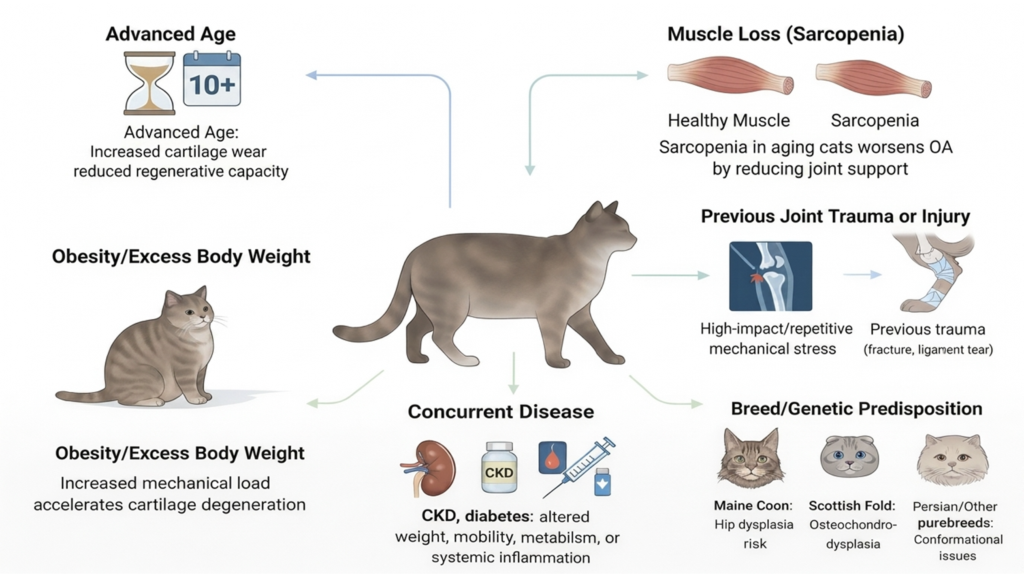
Risk Factors for Feline OA
In contrast to the dog, where well-defined predisposing arthropathies (hip dysplasia, elbow dysplasia, cruciate disease, patellar luxation, OCD) account for the majority of clinical OA, a substantial proportion of feline OA is classified as primary or idiopathic, reflecting genuine biological differences as well as our incomplete understanding of feline joint disease7,8,18.
1. Age: The Strongest and Most Consistent Risk Factor
Age is the single most consistently documented risk factor for feline OA. Prevalence rises steeply with age, with most studies reporting that more than 60% of cats over 6 years and approximately 90% of geriatric cats have radiographic evidence of appendicular OA1,3–5,9. However, structural changes consistent with OA have been documented in cats as young as 1 year of age.8
2. Breed and Genetic Predisposition
Breed-specific predisposition in cats is less extensively characterized than in dogs, but several patterns are now well established:
- Scottish Fold osteochondrodysplasia: Caused by a missense mutation (V342F) in TRPV4, the same gene that produces the breed’s characteristic folded ears. Cartilage is abnormal throughout the body, and all Scottish Folds with folded ears develop osteochondrodysplasia and progressive, crippling polyarticular OA—earliest and most severe in homozygotes, milder but still inevitable in heterozygotes19,20.
- Maine Coon hip dysplasia: A long-running radiographic health-screening program in over 5000 Maine Coons reported a prevalence of 37.4% for feline hip dysplasia (FHD) and a positive genetic correlation between FHD severity and body mass, indicating that selection for the breed’s characteristic large body size has selected for FHD21.
- Persian, Himalayan, and Devon Rex hip dysplasia: Reported prevalences in purebred cohorts approach 24%, compared with approximately 10% in domestic shorthairs21,22.
Beyond these specific syndromes, gene-expression studies strongly suggest that broader genetic variation in immune, apoptotic, and pain-signaling pathways modulates the development and clinical expression of feline DJD.11,17 This highlights how OA in cats is truly an individualized disease based on unique genetic markers and risk factors. The candidate gene catalog in feline OA, however, remains markedly less developed than in the dog or human.
3. Previous Trauma and Joint Injury
Cats are uniquely exposed to high-energy trauma including falls from height (“high-rise syndrome”), motor vehicle injuries, bite wounds, and articular fractures that can initiate secondary OA. Approximately 25% of feline OA has been attributed to identifiable prior trauma1,7,9. Feline cranial cruciate ligament rupture is uncommon and, unlike its canine counterpart, is usually traumatic rather than degenerative in origin; nevertheless, it reliably initiates stifle OA when it occurs. Even successfully managed orthopedic cases progress to some degree of OA over time, which is why post-injury joint surveillance is part of long-term feline care.
4. Comorbid Disease (particularly Chronic Kidney Disease)
No discussion of feline OA risk and management is complete without addressing the striking co-prevalence of OA and chronic kidney disease (CKD). A retrospective study demonstrated that approximately 68% of cats diagnosed with OA had concurrent CKD, with significant concurrence between the two diseases across all age groups23. The mechanisms linking the two are likely bidirectional and only partially understood. Reduced mobility from painful OA may reduce voluntary water intake and predispose to subclinical dehydration; chronic inflammation associated with OA may contribute to tubulointerstitial injury; and shared age-related and immune-inflammatory mechanisms may drive both processes in parallel.
Proteomic profiling of cats with DJD + pain and DJD + pain + CKD demonstrated similar alterations, and in cats with concurrent CKD, additional changes were identified associated with IL-12 signaling and production in macrophages12. Findings suggested that chronic, low-grade, macrophage-driven inflammation is a common mechanism for both diseases, rather than coincident comorbidity in an aging population12.
5. Body Weight/Obesity
The role of body weight in feline OA is more equivocal than in dogs. Some cross-sectional studies have failed to demonstrate a significant association between body condition score and radiographic OA in cats3, while others, particularly studies focused on the stifle, have shown overweight cats to have a higher prevalence of OA changes24. Two factors likely explain this apparent inconsistency. First, cats rarely reach the extremes of obesity seen in dogs. Second, mechanical load is only one mechanism by which obesity contributes to OA; the systemic adipokine-mediated inflammatory contribution is mechanistically plausible in cats but has been studied far less than in dogs or humans8. Leptin, a major adipokine implicated in human and canine OA, has not yet been rigorously evaluated in feline OA.
Despite the incomplete mechanistic picture, lean body condition is universally recommended in feline OA management, both because mechanical unloading benefits affected joints and because obesity is independently associated with diabetes mellitus, hepatic lipidosis, and reduced overall mobility, all of which compound the clinical impact of OA in the cat.
6. Sex and Neuter Status
The available feline data do not show a strong, consistent independent effect of sex or neuter status on OA risk. Some studies report increased prevalence in male cats, others report no difference, and most are limited by small sample sizes and confounding with body weight and age3,9. Neutering itself is so close to universal in pet cats in much of the world that disentangling its effect from other variables is difficult. Unlike in some large-breed dogs, there is no compelling evidence in cats that timing of neutering alters OA risk in clinically meaningful ways.
How Feline OA Pathophysiology Changes with Age
OA in the cat is sometimes treated as a single disease state, but its biology and clinical presentation shift substantially across the lifespan.
Young Cats: Developmental and Trauma-Driven Disease
In kittens and young adult cats, OA most often arises as a consequence of developmental cartilage or skeletal disease or as a sequela of articular trauma. Scottish Folds homozygous for the TRPV4 mutation can develop clinically apparent skeletal disease as early as 7 weeks of age and crippling polyarthropathy within the first one to two years19,20; heterozygotes progress more slowly but inevitably. In Maine Coons and other predisposed pedigrees, signs of hip dysplasia–associated pain may emerge in the first 1–2 years of life. The dominant pathological features at this stage are acute inflammation, subchondral pain, and joint capsule strain, with chronic structural changes (severe muscle loss, contracture, ankylosis) less prominent than they will later become.
Adult Cats: Established Disease and Sensitization
By middle age, cats with predisposing arthropathies typically have established radiographic OA characterized by osteophytes (often mild), subchondral sclerosis, intra-articular mineralization, and joint capsule thickening1,9. The disease landscape is now dominated by chronic low-grade synovial inflammation, peripheral and central pain sensitization, and progressive loss of joint range of motion. Cytokine signatures begin to be detectable in serum (IL-4, IL-8, IL-2, TNF-α)14, and neurobiological changes (CX3CL1 and ATF3 upregulation in DRG, altered NGF in spinal cord) are likely established by this stage in chronically affected cats17. Clinically, this is the population most likely to benefit from sustained multimodal management.
Senior and Geriatric Cats: Multi-Joint Disease and Comorbidity
In older cats, OA is most often multi-articular and bilateral. One study found that 91% of randomly selected cats up to 20 years of age had at least one site of appendicular OA4, and approximately half of cats older than 6 years have OA in more than one joint3. Senior cats also accumulate comorbidities—most importantly CKD, but also hyperthyroidism, diabetes mellitus, neoplasia, and cognitive dysfunction that complicate pain assessment and pharmacologic management. The age-related shifts in immune function, apoptosis, and oxidative phosphorylation likely reflect, at least in part, this convergence of multi-organ aging biology on the joint.11
Clinical Implications: Putting Feline OA Pathophysiology to Work
The reframing of feline OA from a passive wear-and-tear process to an active, multi-factorial, whole-joint and whole-body inflammatory disease has direct clinical implications:
- Feline OA is rarely a single-joint problem. Bilateral and multi-joint involvement is the rule, not the exception, which is why cats so rarely show overt lameness. Behavioral changes—reluctance to jump, altered grooming, withdrawal, altered litter box use—are often the only signs and must be actively elicited from caregivers using validated checklists.
- Radiographs and clinical signs do not correlate cleanly. Diagnosis in cats is a combination of orthopedic examination, owner-reported behavioral change, and imaging. Severe radiographic changes can be present in cats with seemingly normal behavior, and vice versa. This will be discussed in more detail in Feline Osteoarthritis Educational Series 2: Diagnosis of OA in the cat
- The molecular biology of feline DJD is genuinely distinct. Feline DJD has a recognizable systemic immunoinflammatory and neuroimmune signature—one that does not map exactly onto canine or human OA.
- Comorbidity often drives management. Concurrent CKD in roughly two-thirds of DJD cats23 may shape analgesic choice. This will be discussed in more detail in Feline Osteoarthritis Educational Series 3: Traditional treatment options for OA in the cat.
- Breed and genetic risk identify cats early. High risk breeds warrant proactive musculoskeletal screening and owner education before clinical signs emerge.
Feline OA is no longer the invisible, untreatable end-of-life condition it was once thought to be. For the veterinary clinician, the modern understanding of feline OA pathophysiology offers something genuinely useful: identifiable mechanisms (some of them species-specific), modifiable risk factors, validated assessment tools, and an expanding therapeutic toolkit—across the lifespan of the cat. Stay tuned for the upcoming installments of the Feline Osteoarthritis Educational Series that review diagnosis, traditional treatment options, and regenerative therapies for cats with OA.
References
- Godfrey DR. Osteoarthritis in cats: a retrospective radiological study. J of Small Animal Practice. 2005;46(9):9. doi:10.1111/j.1748-5827.2005.tb00340.x
- Clarke SP, Mellor D, Clements DN, et al. Prevalence of radiographic signs of degenerative joint disease in a hospital population of cats. Veterinary Record. 2005;157(25):25. doi:10.1136/vr.157.25.793
- Slingerland LI, Hazewinkel HAW, Meij BP, Picavet Ph, Voorhout G. Cross-sectional study of the prevalence and clinical features of osteoarthritis in 100 cats. The Veterinary Journal. 2011;187(3):3. doi:10.1016/j.tvjl.2009.12.014
- Lascelles BDX, Henry Iii JB, Brown J, et al. Cross-Sectional Study of the Prevalence of Radiographic Degenerative Joint Disease in Domesticated Cats: Degenerative Joint Disease in Domestic Cats. Veterinary Surgery. 2010;39(5):5. doi:10.1111/j.1532-950X.2010.00708.x
- Kimura T, Kimura S, Okada J, Suzuki S, Kitanaka T. Retrospective Radiographic Study of Degenerative Joint Disease in Cats: Prevalence Based on Orthogonal Radiographs. Front Vet Sci. 2020;7:138. doi:10.3389/fvets.2020.00138
- Lascelles BDX. Feline Degenerative Joint Disease. Veterinary Surgery. 2010;39(1):2-13. doi:10.1111/j.1532-950X.2009.00597.x
- Bennett D, Zainal Ariffin SMB, Johnston P. Osteoarthritis in the cat: 1. How common is it and how easy to recognise? Journal of Feline Medicine and Surgery. 2012;14(1):1. doi:10.1177/1098612X11432828
- Lefort-Holguin M, Delsart A, Frézier M, et al. Osteoarthritis in cats: what we know, and mostly, what we don’t know. . . yet. Journal of Feline Medicine and Surgery. 2025;27(7):1098612X251347999. doi:10.1177/1098612X251347999
- Bennett D, Morton C. A study of owner observed behavioural and lifestyle changes in cats with musculoskeletal disease before and after analgesic therapy. Journal of Feline Medicine and Surgery. 2009;11(12):997-1004. doi:10.1016/j.jfms.2009.09.016
- Ryan JM, Lascelles BDX, Benito J, et al. Histological and molecular characterisation of feline humeral condylar osteoarthritis. BMC Vet Res. 2013;9(1):110. doi:10.1186/1746-6148-9-110
- Gao X, Lee J, Malladi S, Melendez L, Lascelles BDX, Al-Murrani S. Feline degenerative joint disease: a genomic and proteomic approach. Journal of Feline Medicine and Surgery. 2013;15(6):6. doi:10.1177/1098612X12470652
- Lascelles BDX, Ponnala R, Kamerling SG, Williams T. Proteomic profiling of serum in cats with naturally occurring degenerative joint disease and co-morbid conditions. Front Pain Res. 2025;6:1501932. doi:10.3389/fpain.2025.1501932
- Haseeb A, Haqqi TM. Immunopathogenesis of osteoarthritis. Clin Immunol. 2013;146(3):185-196. doi:10.1016/j.clim.2012.12.011
- Gruen ME, Messenger KM, Thomson AE, et al. Evaluation of serum cytokines in cats with and without degenerative joint disease and associated pain. Veterinary Immunology and Immunopathology. 2017;183:49-59. doi:10.1016/j.vetimm.2016.12.007
- Guillot M, Taylor PM, Rialland P, et al. Evoked Temporal Summation in Cats to Highlight Central Sensitization Related to Osteoarthritis-Associated Chronic Pain: A Preliminary Study. Eldabe S, ed. PLoS ONE. 2014;9(5):e97347. doi:10.1371/journal.pone.0097347
- Monteiro BP, Lascelles BDX, Murrell J, Robertson S, Steagall PVM, Wright B. 2022 WSAVA guidelines for the recognition, assessment and treatment of pain. J of Small Animal Practice. 2023;64(4):177-254. doi:10.1111/jsap.13566
- Ashwell M, Freire M, O’Nan AT, et al. Characterization of gene expression in naturally occurring feline degenerative joint disease-associated pain. The Veterinary Journal. 2019;243:42-47. doi:10.1016/j.tvjl.2018.11.008
- Hardie EM, Roe SC, Martin FR. Radiographic evidence of degenerative joint disease in geriatric cats: 100 cases (1994–1997). javma. 2002;220(5):5. doi:10.2460/javma.2002.220.628
- Gandolfi B, Alamri S, Darby WG, et al. A dominant TRPV4 variant underlies osteochondrodysplasia in Scottish fold cats. Osteoarthritis and Cartilage. 2016;24(8):1441-1450. doi:10.1016/j.joca.2016.03.019
- Takanosu M, Takanosu T, Suzuki H, Suzuki K. Incomplete dominant osteochondrodysplasia in heterozygous Scottish Fold cats. J of Small Animal Practice. 2008;49(4):197-199. doi:10.1111/j.1748-5827.2008.00561.x
- Low M, Eksell P, Högström K, Olsson U, Audell L, Ohlsson Å. Demography, heritability and genetic correlation of feline hip dysplasia and response to selection in a health screening programme. Sci Rep. 2019;9(1):17164. doi:10.1038/s41598-019-53904-w
- Keller GG, Reed AL, Lattimer JC, Corley EA. HIP DYSPLASIA: A FELINE POPULATION STUDY. Vet Radiology Ultrasound. 1999;40(5):5. doi:10.1111/j.1740-8261.1999.tb00375.x
- Marino CL, Lascelles BDX, Vaden SL, Gruen ME, Marks SL. Prevalence and classification of chronic kidney disease in cats randomly selected from four age groups and in cats recruited for degenerative joint disease studies. Journal of Feline Medicine and Surgery. 2014;16(6):465-472. doi:10.1177/1098612X13511446
- Bonecka J, Skibniewski M, Zep P, Domino M. Knee Joint Osteoarthritis in Overweight Cats: The Clinical and Radiographic Findings. Animals. 2023;13(15):15. doi:10.3390/ani13152427

Vice President of Veterinary Affairs at Gallant
Dr. Rebecca Windsor, DVM, DACVIM, is a board-certified veterinary neurologist with over 20 years of clinical experience and a strong record of scientific publication. She joined Gallant in 2025 and serves as Vice President of Veterinary Affairs.
Dr. Windsor specializes in veterinary regenerative medicine, with a focus on advancing FDA-approved, off-the-shelf mesenchymal stem cell therapies for pets. She develops educational platforms that translate the science, safety, and clinical efficacy of stem cell therapy for veterinary professionals. Since 2019, she has served as a Clinician Scientist at Ethos Discovery, where she leads the neurology research portfolio.


